Anaemia: Physiology, Types and Mechanisms
Anaemia is one of the most common clinical conditions worldwide and occurs when the blood cannot carry enough oxygen to meet the body’s metabolic needs. Although often defined by a low haemoglobin level, anaemia is not a diagnosis, it is a manifestation of an underlying problem. The causes range from nutritional deficiencies and chronic disease to bone marrow disorders and haemolysis.
Because oxygen transport is fundamental to cellular function, even mild anaemia can cause fatigue, breathlessness, and reduced exercise tolerance. Understanding the physiology of anaemia helps to understand patterns on pathology results, appreciate compensatory mechanisms, and identify when a patient’s symptoms warrant urgent escalation.
What You Need to Know
Anaemia is a disorder of oxygen transport, not simply a low haemoglobin number. Red blood cells carry oxygen from the lungs to tissues, and when their number, size, or haemoglobin content is reduced, tissue oxygen delivery falls. This creates a state of chronic cellular hypoxia that affects every organ system, particularly the heart, brain, and muscles.
Anaemia develops through three fundamental mechanisms: reduced red blood cell production, increased red blood cell destruction, or blood loss. Reduced production occurs when the bone marrow lacks the materials or signals needed to make red cells, such as iron, vitamin B12, folate, or erythropoietin from the kidneys. Chronic inflammation also suppresses marrow activity by trapping iron and inhibiting erythropoiesis. Increased destruction, or haemolysis, occurs when red blood cells are destroyed faster than they can be replaced, whether by immune attack, inherited membrane or haemoglobin defects, mechanical trauma, or infection. Blood loss removes red cells directly from the circulation, and when bleeding is chronic, iron stores become depleted, compounding the anaemia.
As haemoglobin falls, the body activates compensatory responses to preserve oxygen delivery:
heart rate increases to move more blood per minute
breathing becomes faster and deeper to raise oxygen uptake
blood flow is redistributed toward vital organs
erythropoietin secretion rises to stimulate red cell production
These responses allow patients with mild or slowly developing anaemia to remain relatively asymptomatic.
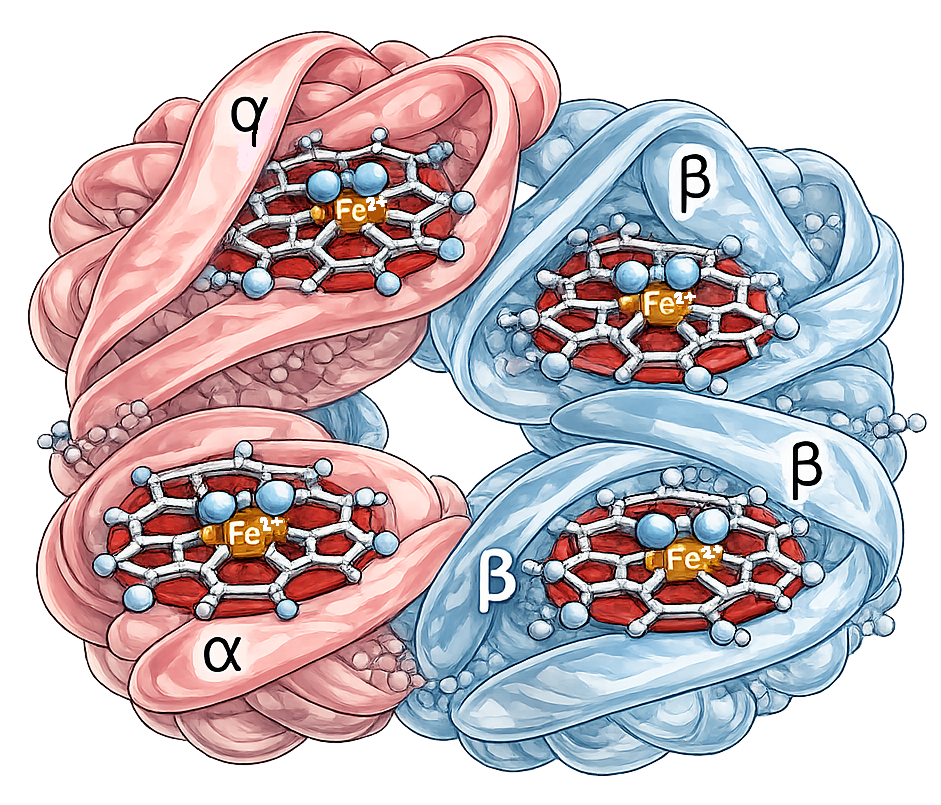
Image: Haemoglobin is a tetramer made up of two alpha (α) and two beta (β) subunits. Each subunit contains a haem group with an iron (Fe²⁺) ion that reversibly binds oxygen (O₂), allowing for efficient oxygen transport.
There are multiple forms of anaemia:
Iron Deficiency Anaemia: Iron deficiency anaemia occurs when iron availability is insufficient for haemoglobin synthesis, leading to reduced oxygen-carrying capacity of red blood cells. It most commonly results from chronic blood loss, inadequate intake, or impaired absorption.
Anaemia of Chronic Disease (Inflammation): Anaemia of chronic disease develops when inflammatory processes suppress red blood cell production and alter iron handling, despite normal or increased iron stores. The bone marrow is unable to effectively utilise available iron, resulting in reduced haemoglobin synthesis.
Vitamin B12 and Folate Deficiency Anaemia: These anaemias occur when impaired DNA synthesis disrupts normal red blood cell maturation, producing large, fragile red cells that are inefficient at oxygen transport. They are commonly associated with malabsorption, dietary deficiency, or increased metabolic demand.
Haemolytic Anaemia: Haemolytic anaemia results from premature destruction of red blood cells, leading to a lifespan shorter than the normal 120 days. Red cell breakdown may be due to intrinsic defects or external factors such as immune attack or mechanical stress.
Aplastic Anaemia: Aplastic anaemia occurs when bone marrow fails to produce adequate red blood cells, often alongside reduced white cells and platelets. This reflects failure of haematopoietic stem cell function rather than increased red cell loss.
Anaemia of Blood Loss: Blood loss anaemia develops following acute haemorrhage or chronic bleeding that gradually depletes red blood cell mass and iron stores. The severity depends on the volume and duration of blood loss.
Anaemia of Chronic Kidney Disease: This form of anaemia arises from reduced erythropoietin production, leading to inadequate stimulation of red blood cell formation. It is often compounded by iron dysregulation and chronic inflammation.
Beyond the Basics
Normal Red Blood Cell Function and Oxygen Transport
Red blood cells are specialised for oxygen transport. They contain haemoglobin, a protein with iron-containing haem groups that reversibly bind oxygen in the lungs and release it to peripheral tissues. Red blood cells are produced in the bone marrow through a tightly regulated process called erythropoiesis and circulate for approximately 120 days before being removed by the spleen. Adequate oxygen delivery depends on multiple factors: sufficient red cell mass, adequate haemoglobin concentration, normal red cell structure, and effective circulation. Anaemia develops when one or more of these elements is compromised.
Reduced Red Blood Cell Production
One major physiological pathway leading to anaemia is impaired erythropoiesis. Red blood cell production requires intact bone marrow function, adequate availability of raw materials, and appropriate hormonal signalling.
Iron is essential for haemoglobin synthesis, while vitamin B12 and folate are required for DNA synthesis during red cell maturation. Deficiency of any of these nutrients results in ineffective erythropoiesis, producing fewer or structurally abnormal red blood cells.
Erythropoietin, a hormone primarily produced by the kidneys, stimulates red blood cell production in response to tissue hypoxia. In conditions such as chronic kidney disease, reduced erythropoietin production leads to anaemia despite adequate iron stores. Similarly, chronic inflammation suppresses marrow responsiveness and alters iron handling, reducing red cell output even when iron intake appears sufficient.
Increased Red Blood Cell Destruction
Anaemia can also result from premature destruction of red blood cells, a process known as haemolysis. When red cells are destroyed faster than the bone marrow can replace them, circulating red cell mass declines.
Haemolysis may occur due to intrinsic red cell defects, such as membrane or enzyme abnormalities, or due to extrinsic factors, including immune-mediated destruction, mechanical damage, or exposure to toxins. Accelerated red cell breakdown increases bilirubin production and places additional metabolic load on the liver and spleen. Even when the bone marrow responds appropriately by increasing production, ongoing haemolysis can overwhelm compensatory mechanisms and result in persistent anaemia.
Blood Loss and Volume Depletion
Acute or chronic blood loss is another common physiological cause of anaemia. Acute haemorrhage reduces circulating red cell mass and plasma volume simultaneously, leading initially to hypovolaemia. As fluid shifts restore plasma volume, haemoglobin concentration falls, revealing anaemia. Chronic blood loss, such as from gastrointestinal bleeding or heavy menstruation, leads to gradual depletion of iron stores. Over time, iron deficiency limits haemoglobin synthesis and reduces red blood cell production, resulting in anaemia even in the absence of overt bleeding.
Impaired Oxygen Delivery Despite Normal Red Cell Count
Anaemia is not always caused by a reduced number of red blood cells. In some cases, red cell count may be normal, but haemoglobin function is impaired. Conditions that alter haemoglobin structure or reduce its oxygen-binding capacity (such as thalassaemias and sickle cell disease) diminish effective oxygen delivery.
Additionally, abnormal red cell shape or rigidity can impair passage through capillaries, limiting oxygen exchange at the tissue level. In these situations, anaemia reflects functional hypoxia rather than absolute red cell deficiency.
Physiological Compensation for Anaemia
When oxygen delivery falls, the body initiates compensatory responses to maintain tissue oxygenation. Cardiac output increases through elevated heart rate and stroke volume, enhancing oxygen delivery per unit time. Peripheral vasodilation improves blood flow to vital organs, while less critical tissues receive reduced perfusion.
At the cellular level, increased oxygen extraction occurs, and over time, erythropoietin secretion rises to stimulate red blood cell production. These compensatory mechanisms explain why some patients tolerate gradual anaemia relatively well, while others with acute onset deteriorate rapidly. However, compensation has limits. When metabolic demand exceeds compensatory capacity, tissue hypoxia develops, leading to fatigue, dyspnoea, cognitive impairment, and organ dysfunction.
Systemic Consequences of Untreated Anaemia
Persistent anaemia places chronic stress on the cardiovascular system and can precipitate or worsen heart failure, particularly in individuals with limited cardiac reserve. Reduced oxygen delivery affects neurological function, immune competence, and wound healing. In severe cases, prolonged hypoxia leads to multi-organ impairment. The physiological burden of anaemia therefore extends far beyond red blood cells, influencing nearly every body system.
Clinical Connections
Symptoms
Anaemia produces a broad range of symptoms because reduced oxygen delivery affects every organ system. Common features include fatigue, pallor, tachycardia, dizziness, breathlessness, cold extremities, and reduced exercise tolerance. When anaemia becomes severe or develops rapidly, myocardial oxygen supply may become inadequate, leading to chest pain, syncope, or heart failure, particularly in older adults or in those with underlying cardiovascular disease.
Assessment
Because anaemia is a physiological syndrome rather than a single disease, investigation must be systematic and broad. Assessment should include:
dietary intake and risk of iron, B12, or folate deficiency
menstrual history and pregnancy status
gastrointestinal symptoms such as bleeding, weight loss, or altered bowel habit
medication use, including anticoagulants, NSAIDs, and chemotherapy
evidence of chronic inflammatory or renal disease
This approach allows clinicians to identify both nutritional and pathological causes.
Iron deficiency anaemia deserves special attention, particularly in older adults, because it is often a marker of occult blood loss rather than poor diet. Conditions such as colorectal cancer, peptic ulcer disease, and angiodysplasia may present only with gradual iron depletion. For this reason, iron deficiency should always prompt investigation for bleeding rather than being treated in isolation.
Haemolytic anaemias can present acutely with jaundice, dark urine, and rapid haemoglobin decline, reflecting accelerated red cell destruction. These conditions can lead to life-threatening anaemia and require urgent recognition and treatment.
Treatment
Treatment depends on the underlying cause and can range from improving diet, taking supplements, such as iron tablets, folate or Vitamin B12, to transfusions and surgery to treat known bleeding. Blood transfusion may be necessary when anaemia is severe or symptomatic, but it does not correct the underlying cause. Understanding the physiological mechanism, whether impaired production, increased destruction, or blood loss, is essential for selecting appropriate long-term therapy and preventing recurrence.
Concept Check
What are the three major physiological mechanisms that cause anaemia?
Why does iron deficiency produce microcytic cells?
How does the body compensate when haemoglobin levels fall?
What pathology findings point toward haemolysis?
Why must iron deficiency anaemia always be investigated rather than simply treated?