Acute Pancreatitis
Acute pancreatitis is an acute inflammatory condition caused by premature activation of digestive enzymes within the pancreas, leading to autodigestion of pancreatic tissue. Unlike pancreatic insufficiency, which results from chronic loss of exocrine function (cannot produce or secrete digestive enzymes), pancreatitis results from acute enzymatic injury with the potential for rapid systemic deterioration. Acute pancreatitis can range from mild, self-limiting inflammation to life-threatening multi-organ failure.
What You Need to Know
Acute pancreatitis develops when the normal protective mechanisms that separate pancreatic enzyme production from enzyme activation fail. Under normal physiological conditions, digestive enzymes are synthesised in an inactive form and activated only after they reach the small intestine. In acute pancreatitis, premature activation occurs within the pancreatic tissue itself, allowing enzymes to digest pancreatic cells, blood vessels, and surrounding fat. This autodigestion triggers intense local inflammation and rapidly compromises pancreatic structure and function.
Pancreatitis can develop as a result of several underlying conditions or triggers that disrupt the normal function of the pancreas. In many cases, these factors contribute to obstruction of pancreatic secretions, direct injury to pancreatic tissue, or premature activation of digestive enzymes within the pancreas itself. Identifying the underlying cause is important, as it may influence both treatment and strategies aimed at preventing recurrent episodes.
Gallstones(can obstruct the common bile duct or pancreatic duct, preventing pancreatic enzymes from draining normally and promoting enzyme activation within the pancreas).
Excessive alcohol consumption(may alter pancreatic secretions, increase the viscosity of pancreatic fluid, and contribute to direct toxic effects on pancreatic cells).
Hypertriglyceridaemia(very high triglyceride levels can result in the release of free fatty acids that damage pancreatic tissue and trigger inflammation).
Hypercalcaemia(elevated calcium levels may promote premature activation of pancreatic enzymes within the pancreatic ducts).
Medications(some drugs, including certain antibiotics, immunosuppressants, diuretics, and antiepileptic medications, have been associated with pancreatic inflammation, although the exact mechanisms are not always clear).
Endoscopic retrograde cholangiopancreatography (ERCP)(instrumentation and manipulation of the biliary and pancreatic ducts during the procedure may cause irritation or obstruction, resulting in post-ERCP pancreatitis).
Abdominal trauma(blunt or penetrating injury can directly damage pancreatic tissue and initiate an inflammatory response).
Infections(viral infections such as mumps, as well as some bacterial and parasitic infections, can trigger pancreatic inflammation).
Autoimmune pancreatitis(immune-mediated inflammation causes pancreatic swelling and dysfunction and may occur in association with other autoimmune conditions).
Genetic factors(inherited mutations affecting pancreatic enzyme regulation or duct function may increase susceptibility to recurrent pancreatitis, particularly in younger individuals).
Idiopathic pancreatitis(in some cases, no identifiable cause is found despite thorough investigation).
What begins as a local pancreatic process can quickly evolve into a systemic illness. Activated enzymes and inflammatory mediators increase vascular permeability, allowing fluid to leak out of the intravascular space into surrounding tissues, a process known as third-spacing. The resulting hypovolaemia reduces effective circulating volume and organ perfusion, setting the stage for widespread physiological instability.
Several interacting mechanisms explain why acute pancreatitis can progress from local injury to life-threatening systemic disease:
intrapancreatic enzyme activation leading to tissue destruction and haemorrhage
release of inflammatory mediators that amplify the systemic inflammatory response
fluid shifts and vascular leak causing hypovolaemia and impaired organ perfusion
Disease severity is therefore determined not only by the extent of pancreatic injury but by the magnitude of the systemic inflammatory response and associated fluid losses. Mild cases may remain confined to the pancreas, while severe pancreatitis is characterised by persistent inflammation, circulatory compromise, and the potential for multi-organ dysfunction. Early recognition of this progression is critical, as outcomes are closely linked to the body’s ability to maintain perfusion and limit inflammatory escalation.
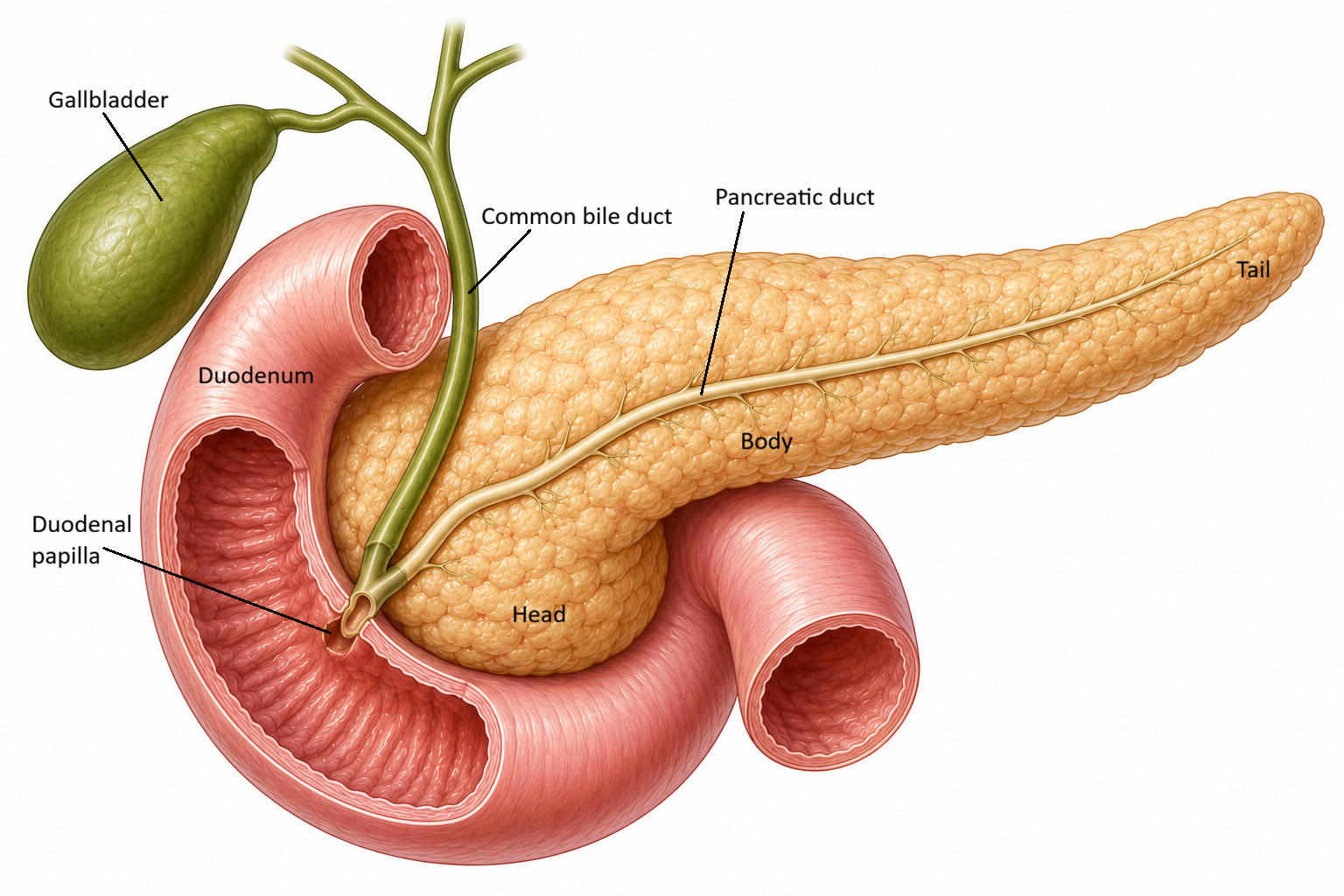
Image: The pancreas drains digestive enzymes into the duodenum through the pancreatic duct, which joins the common bile duct near the duodenal papilla. Obstruction at this shared drainage point, such as by a gallstone, can impair pancreatic outflow and contribute to the development of acute pancreatitis.
Beyond the Basics
Premature enzyme activation and autodigestion
Pancreatic enzymes, such as trypsin, lipase, and elastase, are synthesised to digest dietary fat, protein, and connective tissue rather than pancreatic tissue. Under normal conditions, many of these enzymes are released in inactive forms and remain separated from pancreatic cells until they reach the duodenum. There, enteropeptidase converts trypsinogen into trypsin. Trypsin then activates several other pancreatic enzyme precursors within the intestinal lumen, allowing digestion to occur in the appropriate location. In acute pancreatitis, this protective separation fails and enzymes become activated within the pancreas itself. Premature activation of trypsin is particularly important because it triggers a cascade that activates multiple digestive enzymes within pancreatic tissue, leading to inflammation, cellular injury, and autodigestion of the pancreas.
Once activated, these enzymes digest acinar cells, blood vessels, and surrounding connective tissue. This process of autodigestion is the initiating event in acute pancreatitis and drives all downstream pathology. The pancreas is effectively exposed to the same destructive processes it is designed to apply to food, leading to rapid tissue injury.
Local inflammatory response and tissue necrosis
Enzyme-mediated tissue damage triggers an intense local inflammatory response. Inflammatory cells infiltrate pancreatic tissue and release cytokines, proteases, and reactive oxygen species. This inflammatory environment increases tissue oedema and raises interstitial pressure within the pancreas.
Microvascular blood flow becomes compromised as oedema and inflammation compress small vessels, worsening local ischaemia. Reduced perfusion amplifies cellular injury and promotes pancreatic necrosis. Fat necrosis occurs when lipase digests surrounding adipose tissue, releasing free fatty acids that bind calcium and further amplify inflammation, extending injury beyond the pancreas itself.
Vascular injury and capillary leak
Inflammatory mediators disrupt endothelial integrity, increasing vascular permeability at both local and systemic levels. Plasma leaks from the intravascular space into the retroperitoneum, peritoneal cavity, and surrounding tissues, producing extensive third-spacing of fluid. This capillary leak is a defining feature of acute pancreatitis and explains the rapid intravascular volume depletion seen early in the disease. Significant amounts of fluid can move from the intravascular space into surrounding tissues without obvious external losses, making hypovolaemia difficult to recognise.
Hypovolaemia and reduced organ perfusion
As intravascular volume falls, cardiac output and effective organ perfusion decline. The pancreas itself becomes further ischaemic, which perpetuates enzyme activation and tissue injury, reinforcing a cycle of worsening inflammation and necrosis. Reduced perfusion affects other organs as well. The kidneys are particularly vulnerable, with acute kidney injury developing due to reduced renal blood flow and inflammatory stress. The lungs may also be affected, with increased vascular permeability contributing to pulmonary oedema and acute lung injury.
Systemic inflammatory response
Cytokines and inflammatory mediators released from the pancreas enter the systemic circulation, triggering a systemic inflammatory response. Key mediators include tumour necrosis factor-alpha (TNF-α), interleukins (particularly IL-1, IL-6, and IL-8), platelet-activating factor, nitric oxide, and activated complement proteins. These substances promote widespread endothelial dysfunction, increased vascular permeability, vasodilation, and capillary leak, contributing to intravascular fluid depletion and hypotension. As tissue perfusion becomes compromised, distant organs such as the lungs, kidneys, and cardiovascular system may become affected, increasing the risk of multi-organ dysfunction syndrome (MODS).
Importantly, the severity of systemic illness does not always parallel the degree of pancreatic necrosis seen on imaging. Some patients with limited structural damage develop profound systemic instability, while others with extensive necrosis may initially appear more stable. This highlights the central role of the inflammatory response in determining clinical outcomes, rather than the extent of anatomical damage alone.
Progression to pancreatic insufficiency
Severe or recurrent episodes of acute pancreatitis damage enzyme-producing acinar tissue. With repeated injury, exocrine capacity declines and may not fully recover, leading to chronic pancreatic insufficiency. This progression explains the link between recurrent pancreatitis, malabsorption, and long-term nutritional deficiency. Over time, loss of exocrine function contributes to steatorrhoea, weight loss, and fat-soluble vitamin deficiency, extending the impact of acute pancreatitis well beyond the initial inflammatory episode.
Clinical Connections
Acute pancreatitis is managed as a systemic inflammatory condition rather than an isolated pancreatic disorder, which explains why intravenous fluid resuscitation is central to early treatment. Capillary leak and third-spacing rapidly deplete intravascular volume, even when there is no obvious external fluid loss. Without timely fluid replacement, hypovolaemia worsens pancreatic ischaemia, amplifies intrapancreatic enzyme activation, and accelerates the progression to organ dysfunction. Restoring circulating volume improves pancreatic, renal, and systemic perfusion and reduces the severity of the inflammatory cascade that drives complications.
Several clinical priorities guide early management and reflect the underlying pathophysiology:
aggressive IV fluid administration to counteract third-spacing and maintain effective organ perfusion
adequate analgesia to reduce sympathetic stress responses that further compromise circulation
minimisation of pancreatic stimulation through bowel rest or carefully timed enteral nutrition
Analgesia. Pain control is not only a comfort measure but a physiological intervention. Severe pain reflects pancreatic inflammation, tissue oedema, and irritation of surrounding neural structures, and untreated pain increases sympathetic activation, raising heart rate and peripheral vasoconstriction. This stress response can further impair pancreatic and renal perfusion. Reducing pancreatic stimulation limits further enzyme secretion during the acute phase, which is why early enteral nutrition is introduced cautiously and tailored to disease severity rather than routine oral intake.
Blood Glucose Monitoring. In addition to intravenous fluid replacement and effective analgesia, regular blood glucose monitoring forms an important component of acute pancreatitis management. Inflammation of the pancreas can impair the function of insulin-producing beta cells within the islets of Langerhans, resulting in fluctuations in blood glucose levels. Monitoring allows for the early identification and management of hyperglycaemia, helping to minimise complications associated with poor glycaemic control.
Ongoing assessment focuses on detecting systemic involvement rather than tracking pancreatic injury alone. Changes in urine output, creatinine, oxygenation, and haemodynamic status often signal worsening inflammatory burden or inadequate perfusion before structural complications are evident on imaging.
Haemodynamic Support. In patients who remain haemodynamically unstable despite adequate fluid replacement, vasopressor support, such as noradrenaline (typically only administered in critical areas, such as the intensive care unit), may be required to maintain blood pressure and preserve organ perfusion. Severe cases may necessitate admission to a high dependency or intensive care setting for close monitoring and advanced organ support, including respiratory support, such as high flow oxygen therapy or mechanical ventilation, renal replacement therapy, or ongoing vasopressor therapy.
Acute pancreatitis frequently evolves dynamically over the first 24 to 72 hours, and outcomes are closely linked to how effectively circulatory stability is maintained during this period. Continuous reassessment of fluid balance, organ function, and overall physiological trajectory is therefore central to reducing morbidity and preventing progression to multi-organ dysfunction.
Concept Check
Why does premature enzyme activation initiate pancreatic autodigestion?
How does capillary leak contribute to hypovolaemia in acute pancreatitis?
Why can pancreatitis cause acute kidney injury even without direct renal disease?
How do IV fluids reduce the severity of pancreatic injury?
Why can repeated pancreatitis lead to pancreatic insufficiency?