Absorption Mechanisms: Carbohydrates, Proteins, Lipids, Vitamins & Minerals
Absorption is the final and most clinically significant phase of digestion, as it is the process by which nutrients pass from the gastrointestinal lumen into the bloodstream and lymphatic system to be used by the body’s cells. Without effective absorption, even a perfectly functioning digestive tract cannot support metabolism, growth, repair, or homeostasis. The small intestine is structurally and functionally specialised for this task, with vast surface area, highly selective transport mechanisms, and close integration with the circulatory and lymphatic systems.
What You Need to Know
For nutrients to be absorbed, they must first be broken down into small, transportable units that can cross the intestinal epithelium. The majority of absorption occurs in the jejunum, although the duodenum and terminal ileum play specialised roles in the uptake of specific nutrients. This process is supported by the highly folded structure of the intestinal mucosa, with villi and microvilli forming a dense brush border that dramatically increases surface area and places nutrients in close proximity to transport proteins within enterocyte membranes.
Absorption is not a single uniform process. Different nutrient classes use different transport mechanisms depending on their chemical properties, size, and solubility. These mechanisms determine how efficiently nutrients are absorbed and where they enter the circulation. Broadly, intestinal absorption relies on several key transport strategies:
facilitated diffusion, which moves nutrients down a concentration gradient using membrane transport proteins
secondary active transport, which couples nutrient uptake to ion gradients, most commonly sodium
passive diffusion, used by small or lipid-soluble molecules that cross membranes directly
endocytosis, reserved for a limited number of larger or complex molecules
Once absorbed, nutrients follow different post-absorptive pathways. Water-soluble substances, such as monosaccharides and amino acids, are absorbed directly through the intestinal wall (through villi), into the bloodstream and enter the portal circulation where they are transported directly to the liver for processing. In contrast, most lipids are packaged into chylomicrons (large fat-transporting lipoprotein particles) and transported via the lymphatic system before entering the bloodstream. Together, these mechanisms ensure that carbohydrates, proteins, lipids, vitamins, and minerals are absorbed efficiently while maintaining tight regulation of nutrient delivery to the rest of the body.
Beyond the Basics
Absorption of carbohydrates
Dietary carbohydrates must be reduced to monosaccharides before absorption, with glucose, galactose, and fructose accounting for the majority of carbohydrate uptake. Glucose and galactose enter enterocytes (the primary epithelial cells that line both the small and large intestine, often referred to as the gatekeepers for nutrient absorption) via secondary active transport using sodium-dependent glucose co-transporters on the apical membrane. This process is driven by the sodium gradient maintained by the Na⁺/K⁺ ATPase pump on the basolateral membrane, which indirectly supplies the energy required for uptake. Therefore, a significant sodium imbalance may impair glucose and galactose absorption by disrupting the sodium gradient that drives sodium-dependent co-transport, reducing the efficiency of nutrient uptake across the intestinal epithelium.
Fructose is absorbed by a different mechanism, entering enterocytes via facilitated diffusion through the GLUT5 transporter. Unlike glucose and galactose, fructose absorption does not depend on sodium co-transport and occurs by movement down its concentration gradient.
Absorption of proteins
Proteins are absorbed predominantly as free amino acids, although small dipeptides and tripeptides are also efficiently transported. Amino acids cross the apical membrane (the surface of an epithelial cell that faces the lumen) through multiple carrier-mediated transport systems, many of which are sodium dependent and selectively tuned to different amino acid classes.
Small peptides are absorbed via proton-coupled transporters and are rapidly hydrolysed into free amino acids within the enterocyte. Regardless of their initial form, absorbed amino acids exit the basolateral membrane into the portal circulation and are delivered to the liver, where they contribute to protein synthesis, energy production, or the generation of other nitrogen-containing compounds.
Absorption of lipids
Lipid absorption differs fundamentally from that of carbohydrates and proteins due to the hydrophobic (water-repelling) nature of most lipids. Following emulsification by bile salts and enzymatic digestion by pancreatic lipase, triglycerides are broken down into free fatty acids and monoglycerides. These products associate with bile salts to form micelles (tiny, ball-shaped clusters formed by molecules that are both water-loving and oil-loving), which facilitate diffusion across the apical membrane of enterocytes.
Within the enterocyte, fatty acids and monoglycerides are reassembled into triglycerides and packaged with proteins to form chylomicrons (large, fat-transporting lipoprotein particles). Because of their size, chylomicrons cannot enter blood capillaries and instead pass into intestinal lymphatic vessels known as lacteals. They are transported through the lymphatic system and enter the systemic circulation via the thoracic duct, initially bypassing hepatic metabolism.
Short-chain fatty acids represent an exception to this pathway, as they are sufficiently water soluble to diffuse directly into the portal circulation without chylomicron formation.
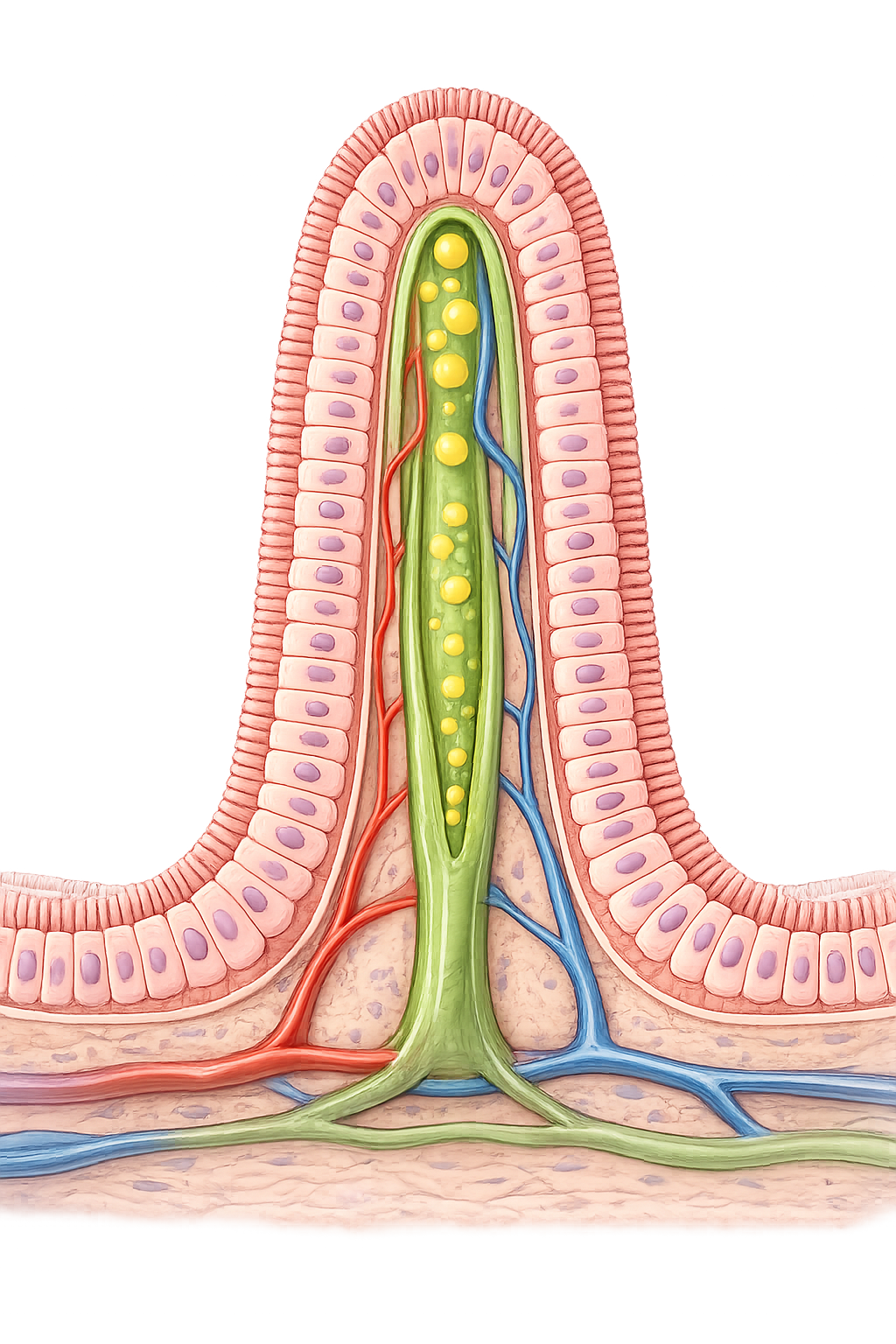
Image: Lacteals are specialised lymphatic capillaries located within the centre of intestinal villi. Unlike carbohydrates and amino acids, dietary lipids are absorbed into lacteals as chylomicrons and transported through the lymphatic system before entering the bloodstream.
Absorption of vitamins
Water-soluble vitamins, including the B-complex group and vitamin C, are absorbed primarily through carrier-mediated transport and diffusion, with most uptake occurring in the jejunum. Vitamin B₁₂ requires a specialised mechanism involving binding to intrinsic factor in the stomach, followed by receptor-mediated endocytosis in the terminal ileum. Without intrinsic factor, efficient B₁₂ absorption cannot occur.
Fat-soluble vitamins A, D, E, and K are absorbed alongside dietary lipids within micelles and incorporated into chylomicrons. Their absorption is therefore dependent on adequate bile secretion and pancreatic enzyme activity, linking vitamin uptake directly to normal fat digestion.
Absorption of minerals and electrolytes
Mineral absorption is tightly regulated and varies according to physiological demand. Iron is absorbed primarily in the duodenum via specialised transporters, with absorption rates increasing when body iron stores are depleted. Once absorbed, iron binds to transferrin for transport in the bloodstream.
Calcium absorption occurs mainly in the duodenum and jejunum and is strongly influenced by vitamin D, which increases expression of calcium transport proteins. Sodium absorption plays a central role in driving the uptake of many other nutrients and water, while chloride generally follows passively. Potassium is absorbed largely by diffusion, and minerals such as magnesium and phosphate use a combination of passive and active mechanisms depending on dietary load and systemic requirements.
Water absorption and fluid balance
The gastrointestinal tract absorbs several litres of fluid each day, the majority of which originates from digestive secretions rather than ingested liquids. Water movement is passive and follows solute absorption, particularly sodium, by osmosis. The small intestine is responsible for most water absorption, while the large intestine fine-tunes fluid and electrolyte balance before waste elimination.
Disruption of water absorption rapidly leads to dehydration, electrolyte imbalance, and circulatory compromise, highlighting the importance of coordinated solute transport for maintaining overall fluid homeostasis.
Integration with circulation and metabolism
Most absorbed nutrients enter the hepatic portal circulation and are delivered directly to the liver, allowing immediate regulation of glucose, amino acids, and many electrolytes before they reach systemic circulation. This first-pass processing plays a central role in metabolic control.
Lipids follow a different route, entering the circulation through the lymphatic system and bypassing the liver initially. This dual routing reflects fundamental differences in nutrient chemistry and metabolic handling, ensuring that absorption and distribution are matched to physiological need.
Clinical Connections
Disorders of intestinal absorption lead to malnutrition even when dietary intake is adequate, because nutrients cannot be effectively transferred across the intestinal epithelium. The clinical consequences depend on which absorptive mechanisms are disrupted and which regions of the intestine are affected, often producing characteristic patterns of deficiency.
Structural damage to the mucosa has a profound impact on nutrient uptake. In coeliac disease, immune-mediated villous atrophy markedly reduces absorptive surface area, impairing uptake of carbohydrates, proteins, fats, vitamins, and minerals. Pancreatic insufficiency disrupts fat digestion by limiting lipase delivery, resulting in steatorrhoea, weight loss, and deficiency of fat-soluble vitamins. Similarly, bile duct obstruction prevents effective fat emulsification, further compromising lipid and vitamin absorption.
Common clinical manifestations of impaired absorption include:
weight loss and failure to thrive despite adequate oral intake
fat-soluble vitamin deficiency presenting with bone disease, coagulopathy, or visual disturbance
anaemia, particularly iron deficiency or vitamin B₁₂ deficiency
chronic diarrhoea and steatorrhoea due to unabsorbed nutrients remaining in the intestinal lumen
Micronutrient deficiencies often reflect absorptive failure rather than dietary shortage. Iron deficiency anaemia most commonly arises from impaired absorption in the duodenum, while vitamin B₁₂ deficiency results from loss of intrinsic factor secretion or dysfunction of the terminal ileum, leading to haematological and neurological consequences if untreated.
Severe diarrhoea overwhelms normal absorptive capacity and rapidly depletes fluid and electrolytes. This is particularly dangerous in infants, older adults, and medically compromised patients, where even short periods of impaired absorption can lead to dehydration, electrolyte imbalance, and circulatory instability.
Concept Check
Why do glucose and galactose require sodium for absorption but fructose does not?
Why must triglycerides be transported via the lymphatic system?
Why does vitamin B₁₂ require a special absorption mechanism?
Why does bile obstruction lead to fat-soluble vitamin deficiency?
Why does sodium absorption drive water absorption in the intestine?