Burn Depth: Progressive Tissue Destruction and Loss of Regenerative Capacity
Burns vary in severity not only by surface area, but by depth of tissue involvement. Burn depth reflects the extent of cellular destruction, vascular damage, and loss of regenerative structures, and is a key determinant of healing potential, complication risk, and long-term outcomes. Understanding the pathophysiology of burn depth explains why some burns heal spontaneously, why others require surgical intervention, and why deeper burns are associated with greater systemic stress even when surface area appears limited.
What You Need to Know
Burn depth describes the extent to which thermal injury penetrates through the layered structure of the skin and determines the tissue’s capacity for recovery. The epidermis provides the primary barrier, while the dermis contains blood vessels, nerves, sweat glands, hair follicles, and stem cell populations essential for regeneration. As injury extends deeper, these regenerative structures are progressively damaged or destroyed, shifting healing from restoration toward scarring.
Depth is therefore not simply a descriptive label but a reflection of biological viability. Superficial injury preserves blood supply and epithelial stem cells, allowing re-epithelialisation to occur. Deeper injury compromises perfusion, sensation, immune defence, and repair capacity, increasing the risk of infection, fluid loss, and long-term functional impairment. Importantly, burn depth can evolve over time as ischaemia, inflammation, and oedema extend tissue injury beyond the initial thermal insult.
Several key processes explain why increasing depth fundamentally alters healing potential:
Progressive loss of epidermal and dermal stem cell reservoirs needed for regeneration
Destruction of dermal blood supply, limiting oxygen delivery and immune access
Transition from epithelial repair to fibroblast-driven scarring as the dominant healing mechanism
As regenerative capacity declines, healing becomes slower, less organised, and more dependent on external support such as surgical intervention or grafting. Deeper burns also act as a persistent inflammatory stimulus, amplifying systemic stress and increasing susceptibility to infection. Burn depth therefore represents a continuum of tissue viability and repair potential, with deeper injury marking a shift from recoverable skin damage to permanent loss of normal skin structure and function.
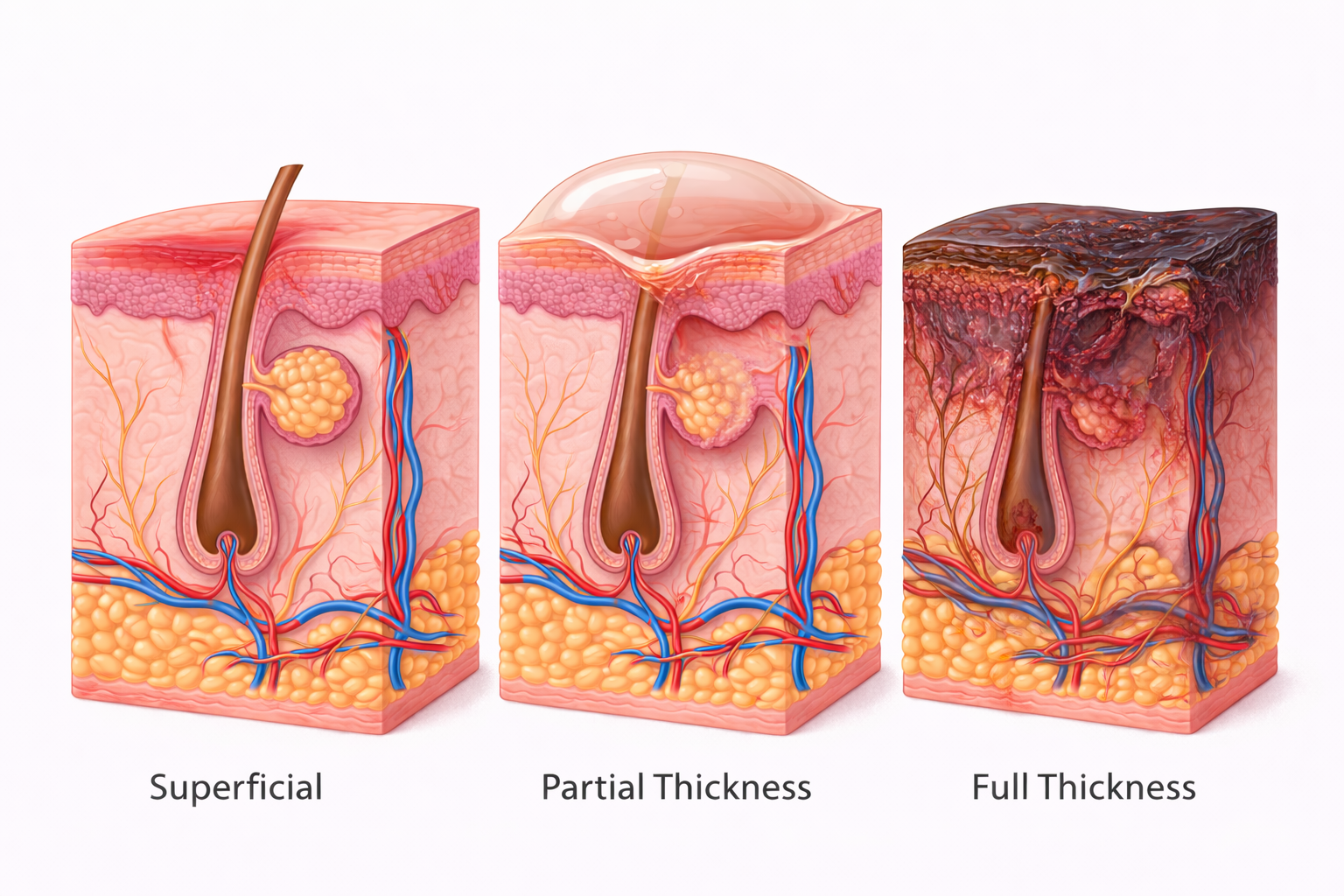
Image: Burns are classified by depth of tissue injury. Superficial burns involve only the epidermis, partial thickness burns extend into the dermis and may form blisters, and full thickness burns destroy the entire dermis and underlying structures, impairing the skin’s ability to regenerate.
Beyond the Basics
Epidermal injury and superficial burns
Superficial burns are confined to the epidermis, where keratinocytes are damaged but the basal layer remains largely intact. Because epidermal stem cells are preserved and dermal structures are unaffected, the skin retains full regenerative capacity. Re-epithelialisation occurs quickly as basal cells proliferate and migrate to restore the surface layer. Vascular integrity remains intact, inflammation is limited, and healing occurs without scar formation. Pain is often prominent because sensory nerve endings in the dermis remain functional and exposed inflammatory mediators heighten nociceptive signalling.
Partial-thickness injury and dermal involvement
Partial-thickness burns extend into the dermis, disrupting blood vessels, connective tissue, and nerve endings to varying degrees. When injury is limited to the superficial dermis, hair follicles and sweat glands remain viable, providing epithelial stem cells that support regeneration and allow healing without grafting if perfusion is adequate and infection is prevented. As injury extends deeper, progressive loss of microvasculature and regenerative units impairs oxygen delivery and delays epithelial migration. Oedema and inflammation further compromise perfusion, prolonging healing and increasing scarring risk. Pain may be severe initially but can diminish as dermal nerve endings are damaged.
Loss of regenerative structures in deep burns
The dermis contains the structural and cellular framework required for effective skin regeneration, including hair follicles, sebaceous glands, fibroblasts, and extracellular matrix scaffolding. These elements supply both new epithelial cells and the organised support needed for orderly repair. As burn depth increases, these regenerative structures are progressively destroyed, removing the biological capacity for re-epithelialisation. Healing then relies on wound contraction and collagen deposition rather than restoration of normal skin architecture, producing stiff, fibrotic scar tissue rather than functional skin.
Full-thickness injury and tissue necrosis
Full-thickness burns involve complete destruction of the epidermis and dermis, leaving tissue that is avascular and non-viable. Blood vessels thrombose, collagen denatures, and normal tissue architecture is lost. Because epithelial stem cells are absent, spontaneous healing cannot occur. These wounds represent permanent skin loss and require surgical intervention to restore coverage and barrier function. Sensation is often reduced or absent due to nerve destruction, which can delay recognition of injury severity and mask ongoing tissue damage.
Extension beyond the skin
In severe burns, thermal injury extends beyond the skin into subcutaneous fat, muscle, or bone. These tissues have limited tolerance for heat and rapidly undergo necrosis when exposed. Deep tissue involvement substantially increases inflammatory mediator release, infection risk, and metabolic demand. Functional impairment is common due to loss of structural support and contracture formation, and recovery is prolonged. Morbidity reflects not only surface injury but the depth and extent of underlying tissue destruction.
Vascular damage and progressive depth conversion
Burn depth is not always fixed at the time of injury. Thermal damage to dermal microvasculature causes endothelial injury, thrombosis, and impaired perfusion in surrounding tissue that may initially appear viable. Ongoing ischaemia, inflammation, and oedema can convert superficial or partial-thickness burns into deeper injuries over hours to days. This dynamic process explains why early reassessment is critical and why timely perfusion support, oedema control, and wound care directly influence final burn depth and outcome.
Relationship between depth and systemic response
Deeper burns release larger quantities of inflammatory mediators, necrotic debris, and damage-associated molecular signals into the circulation. This amplifies capillary leak, hypermetabolism, immune dysfunction, and organ stress. As a result, burn depth contributes to illness severity independently of total surface area. Even burns with limited extent can produce significant systemic effects when tissue destruction is profound, reinforcing depth as a critical determinant of physiological burden.
Clinical Connections
Burn depth shapes clinical behaviour by determining how much viable tissue, blood supply, and regenerative capacity remain within the wound. Superficial burns retain intact dermal structures and epithelial stem cells, allowing rapid re-epithelialisation with supportive care alone. As depth increases, progressive loss of microvasculature and regenerative units reduces healing potential, increases susceptibility to infection, and shifts repair toward fibrosis rather than restoration of normal skin architecture. Pain patterns also change with depth, as intact nerve endings in superficial burns produce marked pain, while deeper injury may blunt sensation despite greater tissue destruction.
Several features link burn depth directly to management decisions:
Preservation or loss of dermal stem cell reservoirs determines whether spontaneous healing is possible
Degree of vascular damage influences perfusion, inflammation, and infection risk
Extent of non-viable tissue dictates the need for surgical debridement and grafting
Early burn appearance can therefore be misleading. Oedema, inflammation, and evolving microvascular thrombosis may cause initially viable tissue to deteriorate over time, deepening the injury beyond its initial presentation. Ongoing assessment prioritises tissue perfusion, inflammatory progression, and viability rather than surface colour or blistering alone. This approach explains why burn management is dynamic, with repeated reassessment guiding escalation from conservative care to surgical intervention as the true depth and biological behaviour of the injury declare themselves.
Concept Check
Why do superficial burns heal without scarring?
How does dermal involvement affect regenerative capacity?
Why are hair follicles important for burn healing?
Why can burn depth increase over time after the initial injury?
How does deeper tissue injury amplify systemic stress?