Lymphadenitis: Lymph Node Inflammation and Immune Activation
Lymphadenitis is inflammation of one or more lymph nodes resulting from infection, immune activation, or, less commonly, malignant infiltration. It reflects an active immune response within lymph nodes rather than a primary failure of lymphatic drainage. Understanding the pathophysiology of lymphadenitis explains why lymph nodes enlarge and become tender, why symptoms are often localised to drainage regions, and why lymphadenitis can signal both effective immune defence and escalating infection.
What You Need to Know
Lymph nodes act as filtration and immune activation sites, trapping pathogens and presenting antigens to lymphocytes. As lymph flows through the node, immune cells interact with foreign material and initiate a targeted response. When microbial load or immune stimulation increases, lymph nodes recruit additional immune cells, increase local blood flow, and amplify inflammatory signalling to contain and eliminate the threat.
Key features of lymph node response include:
Filtration: lymph nodes trap bacteria, viruses, and cellular debris as lymph passes through
Immune activation: antigen-presenting cells (such as dendritic cells) stimulate lymphocytes to mount a response
Cellular recruitment: increased influx and proliferation of lymphocytes leads to node enlargement
Inflammation: release of cytokines increases vascular permeability and local tissue swelling
Pain: stretching of the capsule and surrounding inflammation stimulates sensory nerves
In lymphadenitis, this normal immune response becomes exaggerated or overwhelmed. Increased cellular activity, vascular permeability, and inflammatory mediator release cause the node to enlarge rapidly, become tender, and sometimes fluctuant if suppuration occurs. As swelling increases, normal lymph flow through the node may be impaired, contributing to further congestion and inflammation. The condition therefore reflects active immune system engagement in response to infection, rather than simple mechanical obstruction of lymphatic drainage.
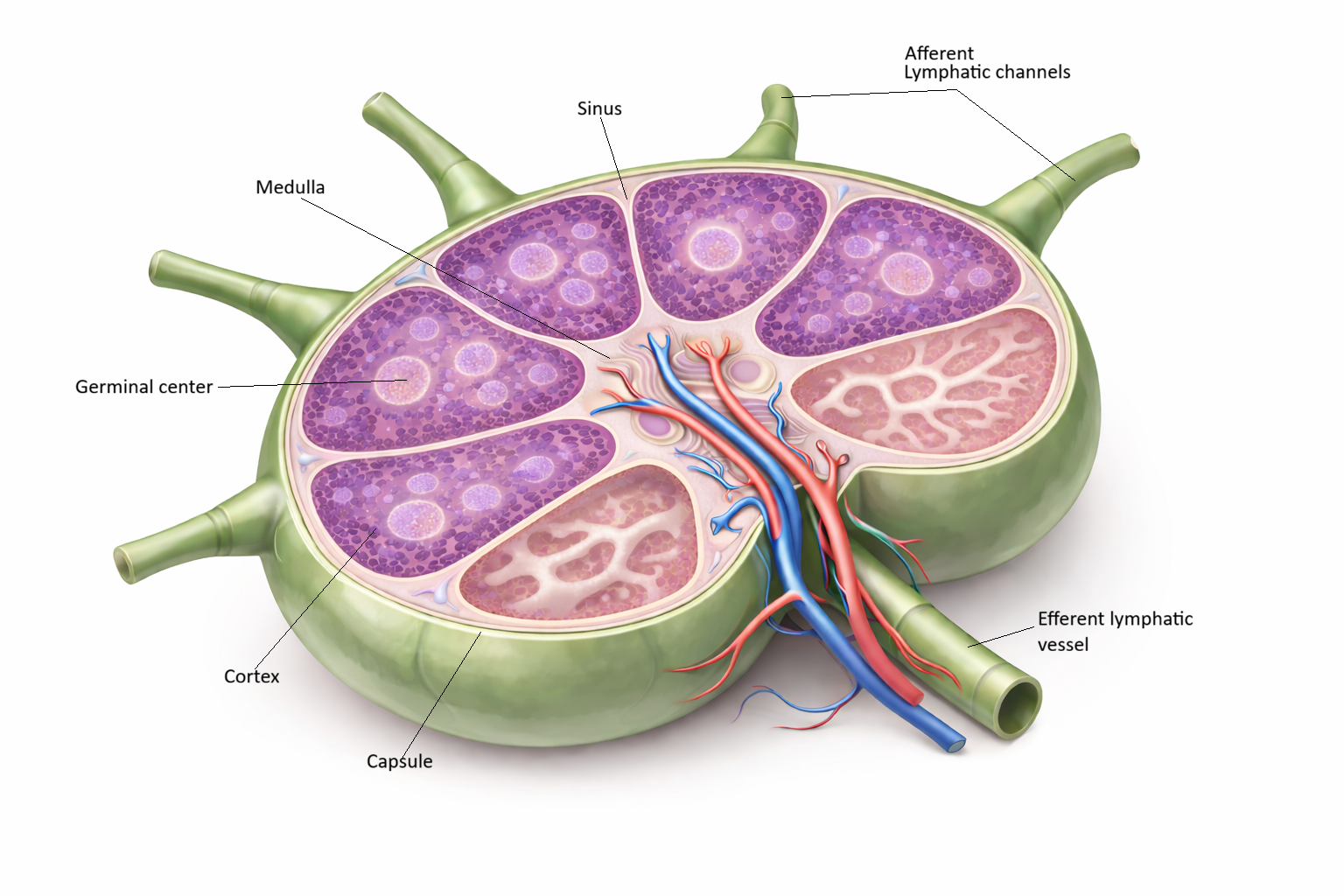
Image: Cross section of a lymph node.
Beyond the Basics
Antigen Trapping and Immune Cell Proliferation
Pathogens entering the lymphatic system are carried in lymph to regional lymph nodes, where they are filtered and processed. Within the node, specialised antigen-presenting cells, such as dendritic cells, display fragments of these pathogens (antigens) to lymphocytes. This interaction activates both B cells (which produce antibodies) and T cells (which coordinate and carry out immune responses), triggering rapid cellular proliferation.
As lymphocytes multiply and accumulate, the overall volume and metabolic activity of the node increase. This is not passive swelling but an active, energy-dependent immune response. Enlargement in this context reflects effective immune engagement, which helps distinguish early lymphadenitis from malignant lymphadenopathy, where enlargement is driven by uncontrolled cellular growth rather than coordinated immune activation.
Inflammatory Oedema and Capsule Stretching
Immune activation within the lymph node is accompanied by increased blood flow and capillary permeability. Cytokines (inflammatory signalling molecules) cause small blood vessels to become “leaky,” allowing plasma proteins and fluid to move into the surrounding interstitial space. This results in oedema within the node.
Lymph nodes are enclosed by a relatively rigid fibrous capsule, so this increase in internal volume raises pressure within a confined space. As the capsule stretches, it stimulates nociceptors (pain receptors), producing the characteristic tenderness of lymphadenitis. This contrasts with many malignant causes of lymph node enlargement, where growth is slower and typically painless due to less acute capsular stretching.
Impaired Lymph Flow and Localised Swelling
As inflammation progresses, the internal architecture of the lymph node becomes congested with proliferating immune cells and excess fluid. This can partially obstruct the normal flow of lymph through the node. Because lymph nodes act as checkpoints along lymphatic vessels, any disruption at this level can affect drainage from upstream tissues.
The result is localised swelling in the region drained by the affected node, due to accumulation of interstitial fluid and increased tissue pressure. In most cases, this impairment is temporary and resolves as inflammation subsides. However, repeated or severe episodes can damage nodal structure and lymphatic channels, increasing the risk of longer-term lymphatic dysfunction.
Suppuration and Abscess Formation
When bacterial load is high or the immune response is unable to effectively contain the infection, neutrophils (a type of white blood cell involved in acute inflammation) accumulate in large numbers. Their enzymatic activity can lead to tissue destruction within the node, resulting in liquefactive necrosis, where solid tissue breaks down into a viscous, fluid-like material.
This process leads to pus formation and the development of a suppurative lymph node or abscess. As pressure builds, the integrity of the node may be compromised, and in some cases, rupture into surrounding tissue can occur. This represents failure of local immune containment and increases the risk of spread to adjacent structures or systemic infection.
Regional Patterns and Source Identification
Lymphadenitis typically occurs in nodes that drain the site of infection, reflecting the directional flow of lymphatic vessels. For example, cervical lymph nodes drain the head and neck, axillary nodes drain the upper limb and breast, and inguinal nodes drain the lower limb and genital region.
This anatomical relationship is clinically useful, as the location of enlarged, tender nodes can provide important clues to the underlying source of infection, even when primary symptoms are mild, resolving, or not immediately apparent. Careful assessment of drainage patterns therefore supports more targeted investigation and management.
Acute vs Chronic Lymphadenitis
Acute lymphadenitis develops rapidly in response to infection and is characterised by tenderness, swelling, and often systemic features such as fever. With effective treatment or resolution of the underlying infection, the inflammatory response subsides and the node typically returns to normal size and function.
Chronic lymphadenitis reflects ongoing or repeated immune stimulation, which may occur with persistent infection, recurrent episodes, or underlying inflammatory conditions. Over time, sustained inflammation leads to fibrosis (replacement of normal tissue with scar-like connective tissue) and distortion of normal nodal architecture. This reduces the node’s ability to filter lymph effectively and increases susceptibility to recurrent infection and lymphatic congestion.
Clinical Connections
Lymphadenitis presents with enlarged, tender lymph nodes, often accompanied by systemic features such as fever and malaise, as well as local signs of infection. The affected node enlarges due to immune cell proliferation and inflammatory oedema, while stretching of the fibrous capsule contributes to pain. In more severe cases, the overlying skin may appear warm or erythematous, reflecting extension of inflammation into surrounding tissues.
Common clinical features include:
Tender lymphadenopathy: pain due to rapid enlargement and capsular stretching
Enlargement: increased nodal size from immune cell proliferation and fluid accumulation
Systemic symptoms: fever, fatigue, and malaise reflecting broader immune activation
Local inflammatory signs: warmth, erythema, and sometimes fluctuance if suppuration develops
Associated infection: symptoms related to the primary source, such as sore throat, skin infection, or wound
Management focuses on identifying and treating the underlying cause. As the primary infection resolves, inflammatory signalling decreases, lymph flow improves, and nodal swelling gradually subsides. Persistent, worsening, or atypical lymphadenitis may indicate complications such as abscess formation or an alternative underlying pathology requiring further assessment.
Concept Check
Why do lymph nodes enlarge during active immune responses?
How does inflammation within a lymph node cause pain?
Why can lymphadenitis impair lymph drainage temporarily?
What distinguishes suppurative lymphadenitis from uncomplicated inflammation?
Why does lymphadenitis often localise to specific anatomical regions?