FRACTURES: Classifications
Fractures are commonly classified using descriptive terms that reflect mechanism of injury, fracture pattern, stability, and tissue involvement. These classifications are not merely descriptive; they provide important insight into the forces involved, expected complications, and healing potential. Understanding fracture types helps explain why some injuries are stable and heal predictably, while others are prone to displacement, vascular compromise, or delayed union. It also supports clearer interpretation of imaging findings and clinical presentations.
What You Need to Know
Fracture classification reflects how bone fails under mechanical stress and provides insight into both injury mechanism and expected healing. The direction, speed, and magnitude of force determine the fracture pattern, while bone quality and surrounding soft tissue influence stability, displacement, and biological repair. In practice, no single classification system captures all aspects of fracture behaviour, so clinicians use a combination of descriptors to build a complete picture.
The main fracture patterns commonly seen are:
Transverse: a horizontal break, usually caused by direct force applied perpendicular to the bone
Stress: a fine hairline crack from repetitive loading and microtrauma rather than a single acute event
Oblique (displaced): an angled fracture often associated with bending forces, frequently with separation of bone ends
Greenstick: an incomplete fracture where one cortex breaks and the opposite side bends, typical in more flexible bone, such as in children
Comminuted: the bone is broken into multiple fragments, usually due to high-energy trauma
Fracture type directly influences biological repair and clinical management. Stable fractures with preserved alignment, intact periosteum, and good blood supply generally heal predictably through organised callus formation. In contrast, unstable or high-energy fractures disrupt vascular supply, increase soft tissue injury, and are more likely to require intervention, with a higher risk of complications such as delayed union, non-union, or infection.
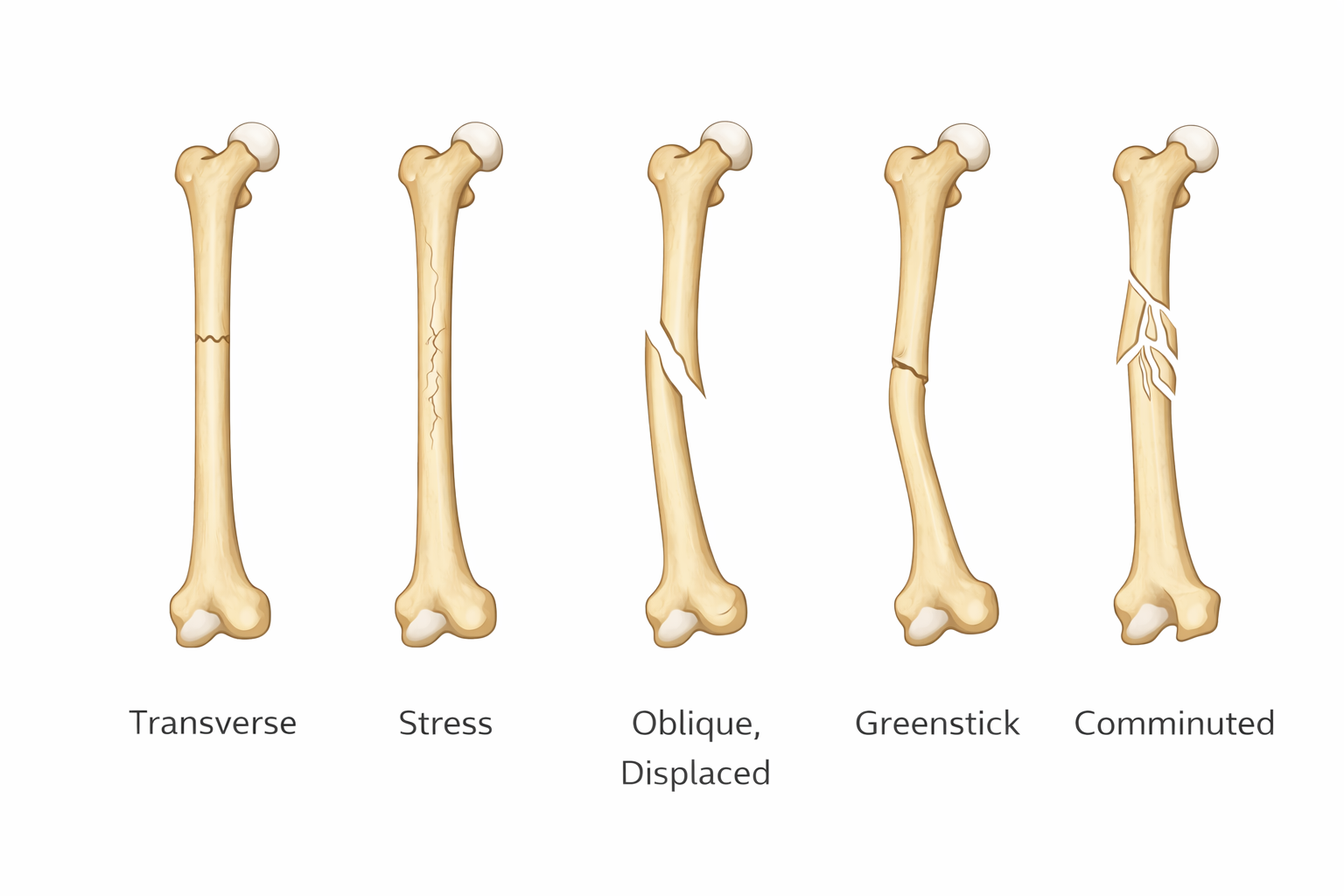
Image: Transverse fractures run straight across the shaft, stress fractures present as fine hairline cracks from repetitive load, oblique displaced fractures occur at an angle with separation of bone ends, greenstick fractures show incomplete cortical failure with bending on the opposite side, and comminuted fractures involve multiple fragmented pieces.
Beyond the Basics
Complete and Incomplete Fractures
A complete fracture extends through the entire cross-section of bone, separating it into two or more distinct fragments. This loss of continuity reduces the bone’s ability to transmit load and often results in instability, particularly when displacement is present. Surrounding soft tissue attachments may be disrupted, which further compromises alignment and blood supply.
Incomplete fractures occur when the bone cracks but does not fully break. These are more common in children because their bones are more elastic and contain a thicker periosteum (the outer connective tissue layer that provides structural support and blood supply). Greenstick fractures involve failure of the cortex on one side with bending on the other, while buckle (torus) fractures result from compressive forces causing the cortex to bulge without a clear fracture line. Although incomplete, both represent structural failure and require appropriate immobilisation to prevent progression or deformity.
Fracture Orientation and Force Direction
Fracture orientation reflects the dominant mechanical force applied to the bone and helps infer the mechanism of injury. Bone behaves differently under compression, tension, bending, and torsion, and the resulting fracture pattern mirrors these stresses.
Transverse fractures occur when bending forces cause failure perpendicular to the long axis of the bone. These fractures may remain relatively stable if the periosteum and surrounding soft tissues are intact. Oblique fractures form when force is applied at an angle, producing a diagonal fracture line that allows fragments to slide past one another, increasing the risk of displacement.
Spiral fractures result from torsional (twisting) forces that create a helical fracture line wrapping around the shaft. This longer fracture surface area reduces inherent stability and increases the likelihood of displacement during movement. Because rotational forces are required, spiral fractures can provide important clues about the injury mechanism.
Displacement and Stability
Displacement describes the loss of normal anatomical alignment between fracture fragments. This may occur as translation (sideways shift), angulation (change in alignment), rotation (twisting of fragments), or shortening (overlap of bone ends). Even small degrees of displacement can alter load distribution across the bone and surrounding joints.
Displaced fractures often disrupt periosteal and endosteal blood supply (the inner vascular network within bone), which is critical for healing. Soft tissue injury further compounds this by increasing inflammation and impairing local perfusion. In contrast, non-displaced fractures maintain alignment and preserve biological conditions for repair.
Stability refers to the ability of a fracture to maintain alignment under physiological load. Stable fractures resist movement and can often be managed conservatively with immobilisation. Unstable fractures tend to shift with minimal stress, increasing the risk of malalignment and impaired healing, and are more likely to require surgical fixation.
Open and Closed Fractures
Closed fractures occur when the skin remains intact over the injury site. While underlying soft tissue damage may still be significant, the intact skin barrier reduces exposure to external contaminants and lowers infection risk.
Open fractures involve a breach in the skin, allowing communication between the fracture site and the external environment. This may occur from bone fragments piercing the skin or from an external object causing both soft tissue and bone injury. These fractures carry a high risk of contamination, infection, and vascular compromise. Urgent management is required to reduce bacterial load, preserve viable tissue, and restore perfusion.
Stress and Insufficiency Fractures
Stress fractures develop when repetitive submaximal loading exceeds the bone’s ability to remodel and repair microdamage. Under normal conditions, bone undergoes continuous remodelling, balancing microdamage with new bone formation. When loading is excessive or recovery is inadequate, microcracks accumulate and eventually coalesce into a fracture. These injuries are common in weight-bearing bones such as the tibia and metatarsals and may initially present with subtle, activity-related pain.
Insufficiency fractures occur when normal physiological stress is applied to bone with reduced structural integrity. Conditions such as osteoporosis (reduced bone density) or osteomalacia (impaired mineralisation) weaken the bone matrix, meaning even everyday forces can result in fracture. These fractures often present insidiously and may be missed without a high index of suspicion.
Comminuted and Segmental Fractures
Comminuted fractures involve the bone breaking into multiple fragments, typically as a result of high-energy trauma. The degree of fragmentation reflects the magnitude of force and is often associated with significant soft tissue injury. Multiple fragments disrupt blood supply and increase the surface area requiring repair, making healing slower and less predictable.
Segmental fractures are characterised by two distinct fracture lines, creating an isolated segment of bone that is no longer connected to the main blood supply at either end. This free-floating segment is particularly vulnerable to impaired healing due to disruption of multiple vascular territories. These fractures are highly unstable and frequently require surgical stabilisation.
Paediatric Fracture Patterns
Children’s bones differ structurally from adult bones, with greater elasticity and a thicker, more biologically active periosteum. This allows bones to absorb more energy before completely failing, resulting in characteristic fracture patterns.
Greenstick fractures occur when tensile forces cause the cortex on one side to fail while the opposite side undergoes plastic deformation (bending without breaking). Buckle fractures result from compressive forces that cause the cortex to bulge outward without a discrete fracture line. Although these injuries may appear less severe radiographically, the underlying biomechanical disruption is significant.
Ongoing growth adds complexity to paediatric fractures. The presence of growth plates (physes) introduces the risk of growth disturbance if injured, and even small alignment issues can lead to progressive deformity over time. Careful assessment and appropriate management are therefore essential to ensure normal bone development.
Clinical Connections
Fracture type influences pain severity, swelling, neurovascular risk, and overall healing trajectory. Injuries involving greater force, displacement, or communication with the external environment cause more extensive soft tissue damage, which directly affects stability and biological repair. Open fractures, displaced fractures, and high-energy mechanisms are therefore associated with higher complication rates, including infection, impaired healing, and neurovascular compromise.
Common terms used in fracture management include:
Reduction: realignment of fracture fragments, either closed (manipulated externally) or open (surgical exposure)
Plaster of Paris (POP): a rigid cast used to immobilise the fracture and maintain alignment
External fixation (ex-fix): stabilisation using pins inserted into bone and connected to an external frame, often used in unstable or open fractures
Internal fixation: surgical stabilisation using plates, screws, or rods applied to or within the bone
Intramedullary nail (IM nail): a rod inserted into the marrow cavity to support long bone fractures
Immobilisation: restricting movement to prevent displacement and allow healing
Weight-bearing status: prescribed (by the treating medical officer) level of load the patient can place through the affected limb during recovery. Examples include non weight-bearing (no weight at all on the affected limb), partial weight-bearing and full weight-bearing
Monitoring for compartment syndrome is essential, particularly in high-energy or tightly enclosed fractures. Increasing pressure within a closed muscle compartment compromises perfusion, leading to ischaemia and potential tissue necrosis. Early signs include pain out of proportion to the injury, pain on passive stretch, and increasing tightness or swelling. Late signs such as pallor, paralysis, and loss of pulse indicate advanced compromise and require urgent intervention.
Stress and insufficiency fractures often present more subtly, with gradual onset pain that is typically activity-related and minimal swelling. Because these injuries can be easily overlooked, particularly early on, they require careful assessment and appropriate imaging when clinical suspicion remains high.
Concept Check
How does fracture orientation reflect the type of force applied to bone?
Why are displaced fractures more likely to have healing complications?
How do stress fractures differ mechanistically from insufficiency fractures?
Why are open fractures considered both skeletal and soft tissue emergencies?
How does bone elasticity influence fracture patterns in children?