The Brainstem: Midbrain, Pons & Medulla
The brainstem is the most primitive and essential region of the central nervous system. It forms the bridge between the spinal cord and higher brain structures and houses the neural circuits responsible for consciousness, breathing, heart rate, blood pressure, swallowing, and reflexive behaviours that sustain life. Although small compared to the cerebrum, the brainstem contains an extraordinarily dense concentration of nuclei, tracts, and cranial nerve pathways. Because of its critical functions, even minor injury to the brainstem can be catastrophic.
What You Need to Know
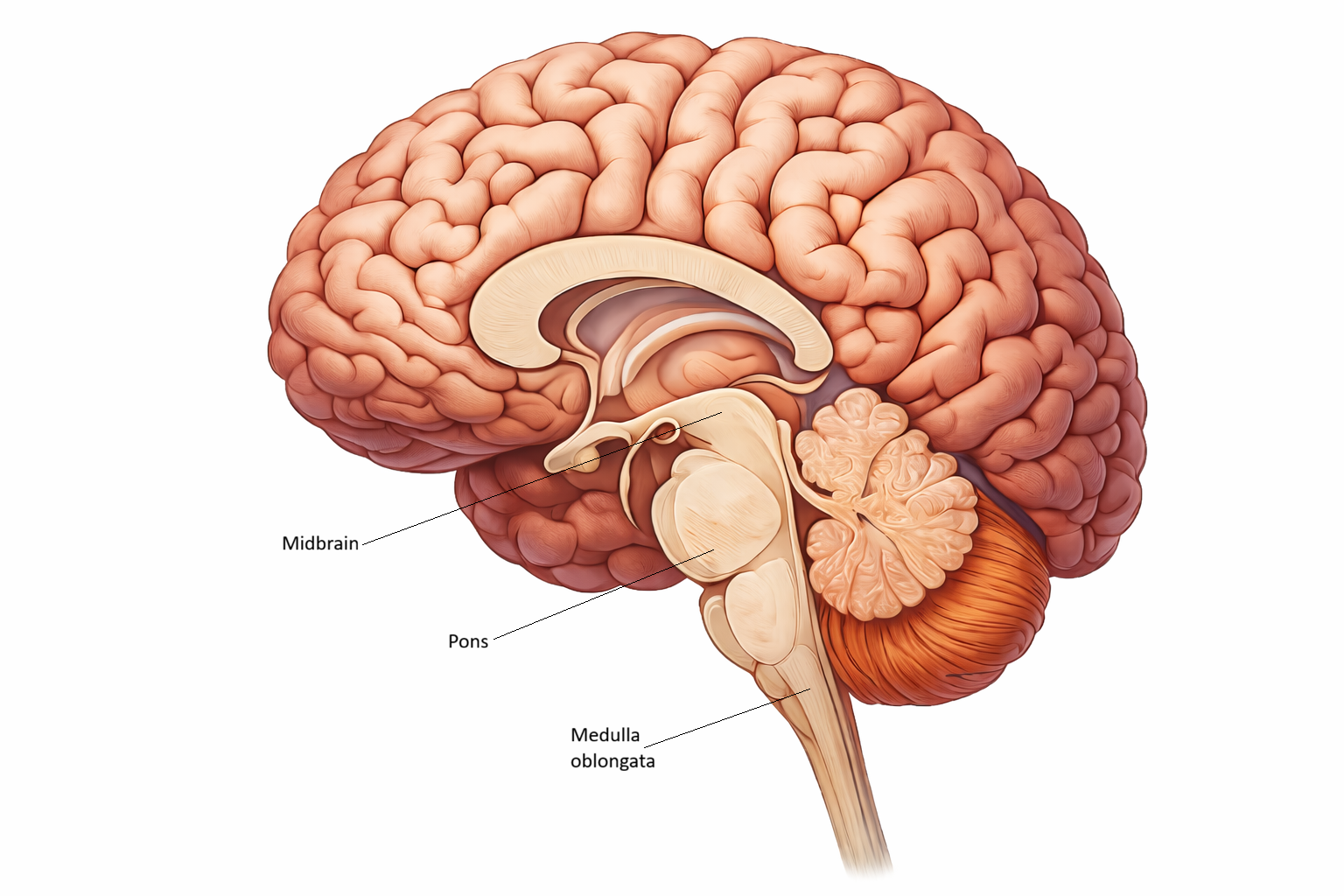
The brainstem consists of three major regions: the midbrain, pons, and medulla oblongata. Together, they contain nuclei for ten of the twelve cranial nerves, ascending sensory pathways, descending motor tracts, and autonomic centres vital for homeostasis.
The midbrain sits just below the thalamus and is responsible for visual and auditory reflexes, eye movements, and the regulation of consciousness through the reticular activating system. It contains the superior and inferior colliculi—structures that coordinate reflexive responses to visual and auditory stimuli. The midbrain also contains the substantia nigra, a key component of the basal ganglia involved in movement regulation.
The pons lies between the midbrain and medulla. It acts as a major relay centre, connecting the cerebrum, cerebellum, and spinal cord. The pons participates in facial sensation, eye movements, chewing, and regulation of breathing rhythm through its pontine respiratory centres.
The medulla oblongata is the lowest part of the brainstem and the transition point into the spinal cord. It contains vital autonomic centres that regulate heart rate, blood pressure, respiratory rhythm, coughing, vomiting, and swallowing. The medulla also houses major ascending and descending tracts, including the pyramidal (corticospinal) pathways where motor fibres decussate.
Beyond the Basics
The Brainstem as a Life-Support Integration Hub
The brainstem is not simply a conduit between the brain and spinal cord. It is a densely packed control centre that integrates consciousness, breathing, cardiovascular function, cranial nerve activity, posture, and reflexes within a structure only a few centimetres long. Nearly every ascending sensory pathway, descending motor tract, and autonomic control system passes through it, making the brainstem one of the most functionally concentrated regions of the nervous system.
Because of this density, even small lesions can produce dramatic and multifaceted neurological deficits. Unlike cortical injuries, which may affect a single domain such as speech or movement, brainstem injury often disrupts multiple life-sustaining systems simultaneously.
Midbrain - Sensory Orientation, Movement Initiation, and Consciousness
The midbrain occupies a pivotal position between the forebrain and hindbrain and plays a central role in orienting the organism to the external world.
The tectum, formed by the superior and inferior colliculi, acts as a sensory integration and reflex centre. The superior colliculus links visual input with head, eye, and neck movements, allowing rapid re-orientation toward moving or threatening stimuli. The inferior colliculus performs a similar function for auditory information, helping the brain localise sound and direct attention toward it.
Beneath this lies the tegmentum, which contains critical motor and arousal nuclei. The substantia nigra and red nucleus are deeply involved in motor control. Dopamine-producing neurons in the substantia nigra modulate basal ganglia circuits that enable smooth, purposeful movement. When these neurons degenerate, as in Parkinson’s disease, movement becomes slow, rigid, and tremulous, reflecting a loss of fine motor control rather than muscle weakness.
The reticular activating system (RAS) runs through the midbrain and upper brainstem, linking sensory input to cortical arousal. This system determines whether sensory information reaches consciousness. Damage to this network reduces alertness, induces stupor or coma, and disconnects the cortex from meaningful sensory input even when the eyes and ears remain intact.
Pons - Coordination of Breathing, Movement, and Facial Function
The pons serves as a communication hub between the cerebrum and cerebellum, allowing voluntary motor plans from the cortex to be refined by the cerebellum before reaching the spinal cord. This makes the pons essential for smooth, coordinated movement and postural control.
It also plays a crucial role in respiratory pattern modulation. While the medulla generates the basic breathing rhythm, pontine nuclei adjust its depth, timing, and smoothness. This fine-tuning allows breathing to adapt to speech, sleep, emotion, and exercise.
Cranial nerve nuclei within the pons control facial sensation, eye movement, facial expression, and aspects of hearing and taste. Damage here produces distinctive patterns of facial weakness, abnormal eye movements, and sensory loss.
Large pontine lesions are especially devastating because they can disconnect the cerebrum from the body while leaving consciousness intact. This produces locked-in syndrome, in which a person is fully aware but unable to move or speak, except through vertical eye movements and blinking.
Medulla - Core Autonomic Control
The medulla contains the most essential autonomic control centres in the entire nervous system. It continuously regulates heart rate, blood pressure, breathing, and airway protection without conscious input.
The dorsal and ventral respiratory groups generate the rhythmic pattern of breathing and adjust ventilation in response to blood gas levels. The cardiac centre and vasomotor centre control heart rate and vascular tone through sympathetic and parasympathetic pathways, allowing blood pressure and cardiac output to adapt to posture, stress, and metabolic demand.
The medulla also houses the nuclei that control swallowing, speech, and airway protection. Reflexes such as coughing, gagging, and vomiting are coordinated here, ensuring that the airway remains clear and that ingested material enters the digestive tract rather than the lungs.
One of the most important anatomical features of the medulla is the pyramidal decussation, where most (85-90%) corticospinal motor fibres cross to the opposite side. The anatomical area is significant because it is why each hemisphere controls the opposite side of the body. This explains why damage above the medulla produces weakness on the opposite side of the body, while damage below produces weakness on the same side.
Why Brainstem Lesions Are So Dangerous
The brainstem’s dense packing of nuclei and pathways means that injury rarely affects just one function. A single lesion can simultaneously disrupt consciousness, breathing, eye movement, swallowing, and motor control.
Midbrain injury commonly produces impaired arousal, abnormal pupils, and movement disorders. Pontine damage can eliminate voluntary movement while sparing awareness. Medullary lesions are often immediately life-threatening because they compromise breathing, cardiovascular control, and airway protection.
Because ascending sensory pathways, descending motor tracts, cranial nerve nuclei, and autonomic centres all converge here, neurological deficits arising from brainstem disease often provide powerful clues about lesion location. This is why careful assessment of eye movements, facial symmetry, voice, swallowing, and breathing is so critical in neurological examination.
The Brainstem as the Nervous System’s Survival Core
The brainstem represents the evolutionary core of the nervous system. It keeps the organism alive, awake, and responsive while higher cortical centres interpret, decide, and plan. Without an intact brainstem, even a perfectly functioning cortex cannot sustain life.
Understanding its anatomy and organisation is therefore fundamental not only to neurology, but to recognising early deterioration, predicting clinical risk, and guiding urgent medical intervention.
Clinical Connections
Because of the dense concentration of life-sustaining nuclei and pathways, brainstem lesions often produce profound neurological deficits.
Common clinical features of brainstem dysfunction include:
Altered level of consciousness (reticular activating system involvement)
Cranial nerve deficits (eye movements, facial weakness, swallowing, speech)
Abnormal pupil size or reactivity
Respiratory pattern changes or failure
Autonomic instability (heart rate, blood pressure dysregulation)
Midbrain lesions may cause impaired consciousness, oculomotor palsies, abnormal pupil responses, and movement disorders.
Pontine lesions can disrupt eye movements, facial expression, and respiratory patterns. Large pontine strokes are notorious for causing locked-in syndrome.
Medullary lesions are particularly dangerous because they can compromise breathing, heart rate regulation, and airway protection. Lateral medullary (Wallenberg) syndrome produces difficulty swallowing, hoarseness, vertigo, sensory loss, and autonomic dysfunction.
Demyelinating diseases such as multiple sclerosis commonly affect brainstem pathways due to their high concentration of myelinated fibres, causing diplopia, facial numbness, vertigo, or impaired coordination.
Trauma can damage the reticular activating system, leading to reduced consciousness or coma. Brainstem compression from raised intracranial pressure is a medical emergency, as it can rapidly impair autonomic function and threaten survival.
Concept Check
Why can small lesions in the medulla cause life-threatening symptoms?
How does the reticular activating system regulate consciousness?
Why do lesions of the midbrain often produce abnormal pupil responses?
What is the significance of the pyramidal decussation in the medulla?
How does the pons contribute to breathing regulation?