The Nervous System - Overview
Disclosure: This article may contain affiliate links. If you purchase through these links, The Nurse Brain may earn a small commission at no extra cost to you. Only trusted resources for nursing education are recommended.
The nervous system is one of the body’s primary communication and control networks. It receives sensory information from the internal and external environment, processes and interprets that information, and coordinates appropriate responses. This system allows us to think, feel, move, maintain homeostasis, and respond rapidly to changing conditions.
The nervous system is broadly responsible for:
Sensory input (detecting changes inside and outside the body)
Integration (processing and interpreting sensory information)
Motor output (sending signals to muscles and glands to initiate a response)
This overview will introduce the major structural divisions of the nervous system, key cell types, and how information is transmitted. Separate posts will cover the autonomic nervous system, synaptic transmission, and higher-order brain functions, as well as the various components of the nervous system with added depth and clinical relevance.
What You Need to Know
The nervous system is the body’s primary communication and control network. It allows the body to sense its environment, process information, and generate appropriate responses. It also coordinates complex functions such as movement, thought, emotion, and regulation of vital organs.
Structurally, the nervous system is divided into two main components:
Central Nervous System (CNS) – the brain and spinal cord
Peripheral Nervous System (PNS) – cranial nerves, spinal nerves, and peripheral nerves
The CNS acts as the integration and decision-making centre. It receives sensory input, processes and interprets this information, and generates motor and autonomic responses. The PNS serves as the communication network, carrying sensory information from the body to the CNS and transmitting motor and autonomic commands back to muscles, glands, and organs.
Functionally, the peripheral nervous system is divided into two major components:
Somatic nervous system – controls voluntary movement of skeletal muscles and carries conscious sensory information such as touch, pain, and temperature
Autonomic nervous system (ANS) – regulates involuntary functions of smooth muscle, cardiac muscle, and glands, and is further divided into the sympathetic, parasympathetic, and enteric systems
The Brain and Spinal Cord (CNS)
The brain and spinal cord form the central nervous system and are protected by the skull, vertebral column, and three layers of meninges (dura mater, arachnoid mater, and pia mater). They are also bathed in cerebrospinal fluid, which cushions and nourishes nervous tissue. The CNS is responsible for processing information, generating movement, regulating vital functions, and supporting higher cognitive processes such as learning, memory, and emotion.
The Brain
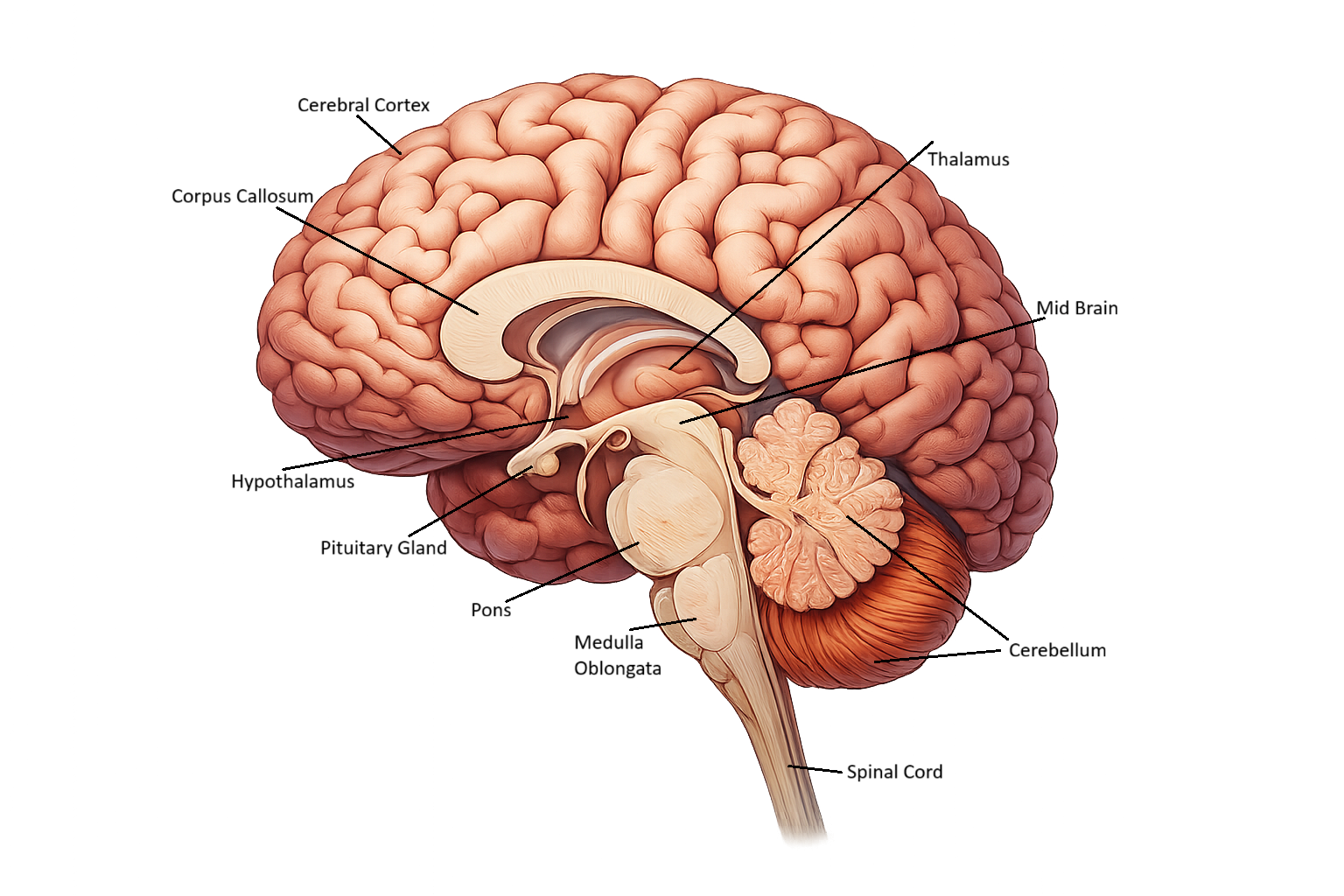
The brain is the command centre of the nervous system. It integrates sensory information, plans and executes movement, regulates autonomic and endocrine function, and supports consciousness and behaviour. It is broadly divided into four major regions:
Cerebrum – responsible for conscious thought, memory, voluntary movement, language, and sensory perception
Diencephalon (thalamus and hypothalamus) – acts as a sensory relay station and regulates homeostasis, including body temperature, hunger, thirst, circadian rhythms, and endocrine activity
Brainstem (midbrain, pons, medulla oblongata) – controls vital functions such as breathing, heart rate, blood pressure, and consciousness, and connects the brain to the spinal cord
Cerebellum – coordinates balance, posture, timing, and precision of movement, allowing smooth and accurate motor control
Lobes of the Brain
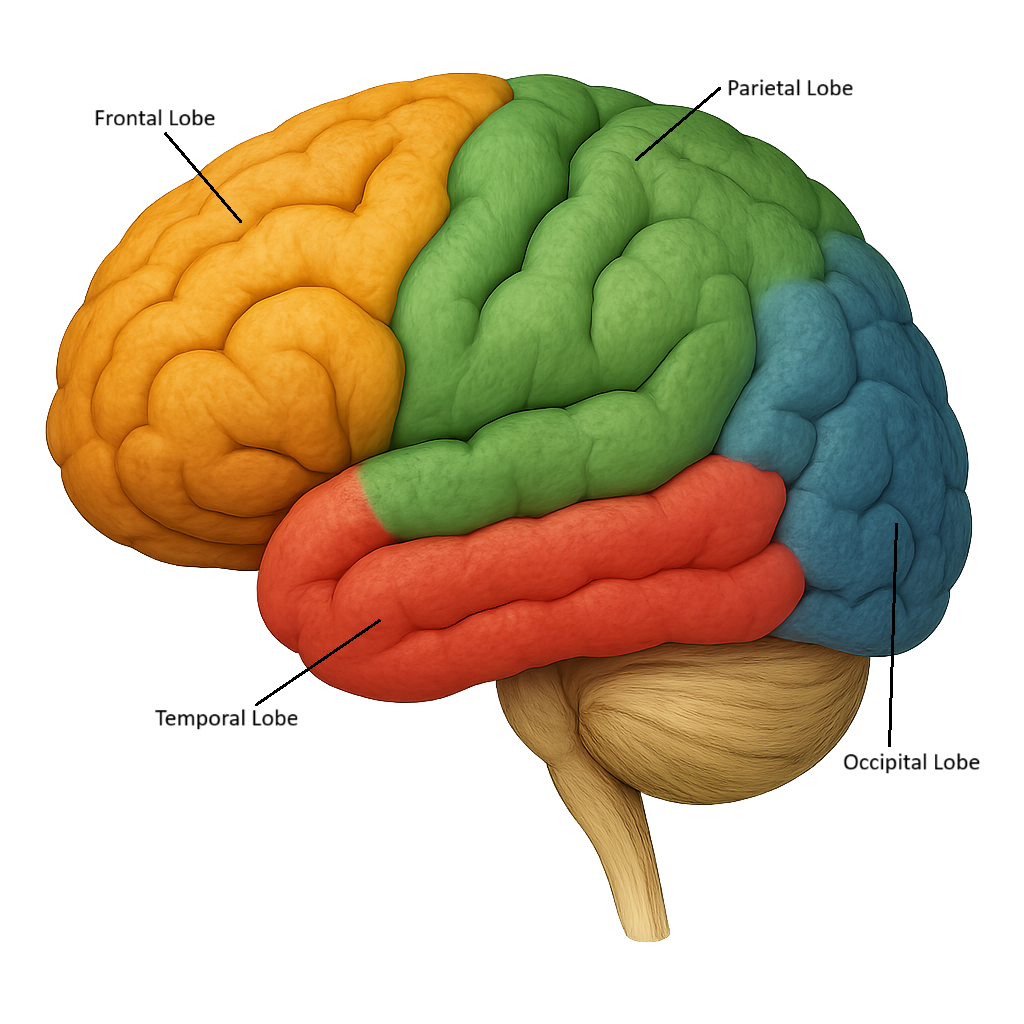
The brain is organised into four main lobes, each with its own location and specialised functions. These lobes help us make sense of what’s happening around us, move our bodies, process information, and create memories. The four lobes are:
Frontal Lobe - The Thinker
Location: front of the brain, behind the forehead
Role: Planning, decision-making, movement, personality, problem-solving, speech. This is the lobe that helps you think ahead and control your actions. It’s also home to the primary motor cortex, which controls voluntary movement.
Parietal Lobe - The Sensor
Location: Top of the brain, behind the frontal lobe
Role: Registers sensations of touch, temperature, pain and spatial awareness. The parietal lobe contains the primary somatosensory cortex, which receives and processes sensations from the body. If you feel something on your skin (ie., a painful sensation), this lobe interprets the sensation.
Temporal Lobe - The Listener and Rememberer
Location: Sides of the brain, near the temples
Role: Hearing, language, memory, emotion. This is where incoming sounds are processed and where many memories are formed. It’s also important in understanding language.
Occipital Lobe - The Vision Centre
Location: Back of the brain
Role: Sight, interpretation of visual information. Everything you see is processed here. Damage to this lobe can affect vision, even if the eyes are healthy.
The Spinal Cord
The spinal cord extends from the base of the brain to around L1–L2 vertebral level. It serves as the main pathway for information travelling to and from the brain. Spinal nerves branch off at each vertebral level, carrying motor and sensory information between the CNS and the body.
The spinal cord also mediates reflexes, which are rapid, protective responses that occur without conscious brain involvement (e.g., withdrawing your hand from a hot surface), also known as a reflex arc.
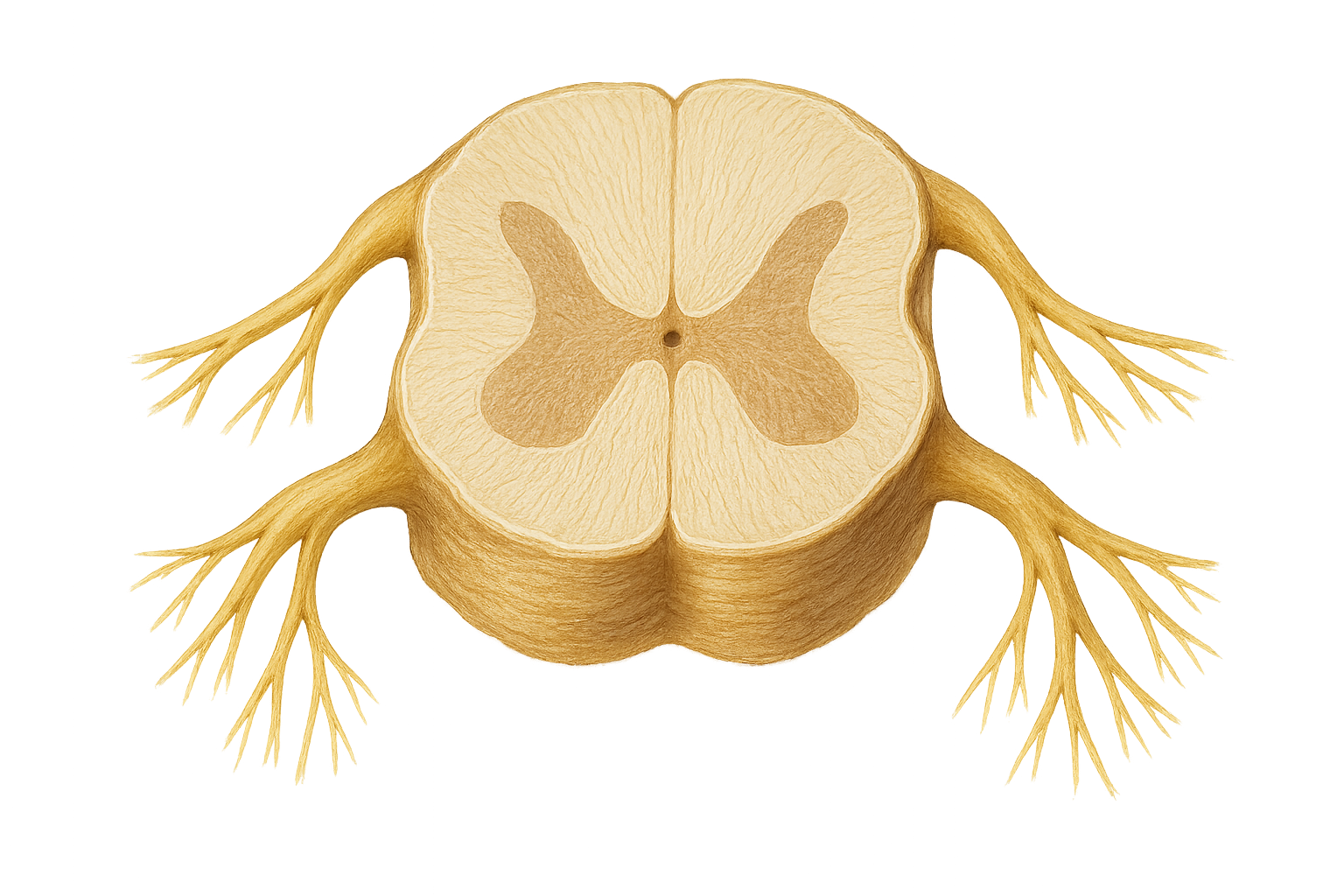
Transverse cross-section of the spinal cord
Nerves, Neurons, and Neuroglia (PNS)
Neurons
Neurons are the functional cells of the nervous system. They generate and transmit electrical impulses (action potentials). Each neuron has:
Dendrites: receive incoming signals
Cell body: integrates information
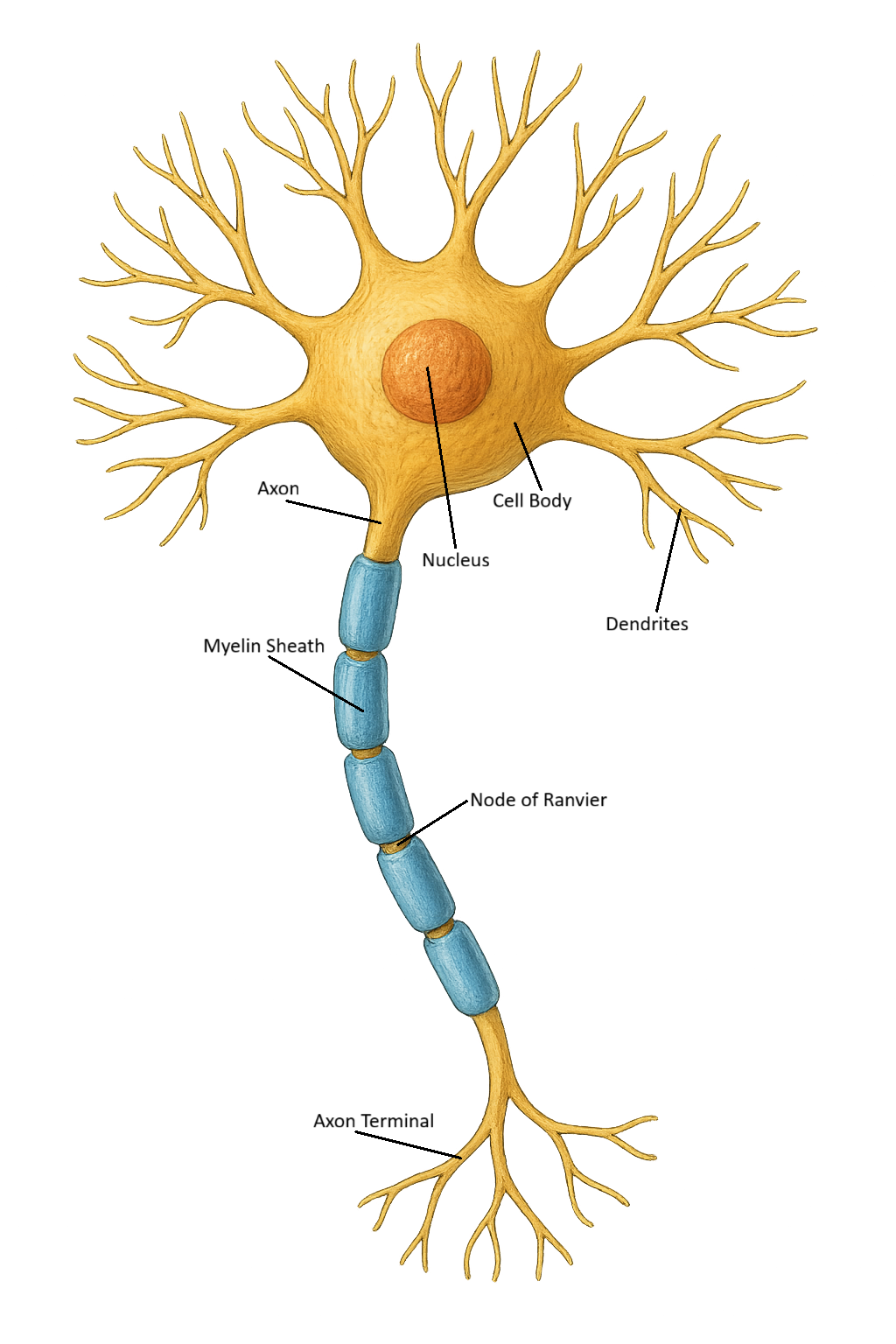
Axon: transmits impulses away from the cell body
Axon terminals: release neurotransmitters to communicate with another cell
Neurons do not divide and are extremely specialised for fast communication.
Neuroglia (Glial Cells)
These are support cells that maintain the nervous system environment. Examples include:
Astrocytes: maintain the blood–brain barrier and regulate nutrients
Oligodendrocytes and Schwann cells: form the myelin sheath, which increases transmission speed
Microglia: act as immune cells within the CNS
Ependymal cells: produce and circulate cerebrospinal fluid
How Information Travels: Action Potentials and Synapses
Neurons communicate through rapid electrical signals known as action potentials. These impulses begin at the axon hillock and travel along the axon, which in many neurons is wrapped in a fatty insulating layer called the myelin sheath. Myelin, produced by oligodendrocytes in the central nervous system, dramatically increases the speed of electrical conduction through a process called saltatory conduction, where impulses “jump” between the gaps in the myelin known as nodes of Ranvier. This allows signals to travel quickly and efficiently over long distances within the nervous system.
When an action potential reaches the axon terminal, it triggers the release of neurotransmitters into the synapse, the small junction between two neurons, or between a neuron and a muscle cell. Neurotransmitters such as acetylcholine, dopamine, glutamate, and GABA bind to receptors on the next cell, creating either:
Excitatory effects – increasing the likelihood that the next neuron will fire
Inhibitory effects – reducing the likelihood of firing, helping to regulate and balance neural activity
This combined system of fast electrical signalling (action potentials) and precise chemical communication (neurotransmitters) the communication process for the nervous system—including thought, memory, sensation, movement, reflexes, mood regulation, and the coordination of complex bodily functions.
Beyond the Basics
Protective Mechanisms of the Nervous System
The nervous system has several key protective structures and processes to safeguard its delicate cells:
Meninges
Between the cerebral cortex and the skull there are three connective tissue layers, each with distinct functions and characteristics. These layers encase the brain and spinal cord, providing physical protection and stability. The layers are the Dura Mater, Arachnoid Mater and Pia Mater, mater meaning ‘mother’ in Latin.
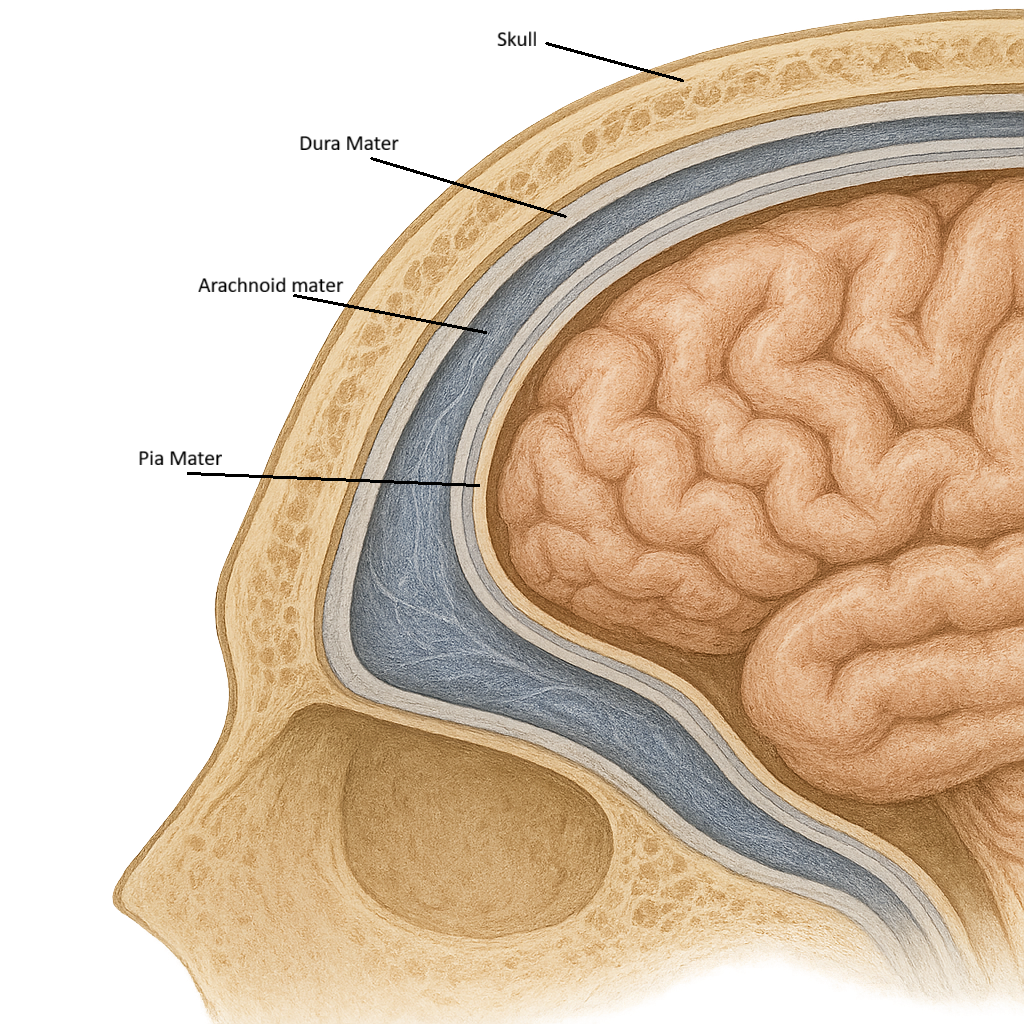
The dura mater, the thick, outermost layer, is shown beneath the skull and contains a rich blood supply, including branches of the middle meningeal artery. Beneath it lies the arachnoid mater, a thin, web-like membrane that does not follow the contours of the brain. The blue subarachnoid space between the arachnoid and pia mater contains cerebrospinal fluid (CSF) and large blood vessels that supply the brain.
The innermost layer, the pia mater, appears as a delicate, pink layer closely adhered to the brain’s surface, following its every fold (gyri) and groove (sulci). Numerous tiny blood vessels can be seen within the pia, demonstrating its role in nourishing the brain tissue directly.
Cerebrospinal Fluid (CSF)
A clear fluid produced by the choroid plexus that:
cushions the brain and spinal cord
helps maintain stable pressure
removes metabolic waste
CSF is a clear, protective fluid that circulates around the brain and spinal cord, filling the ventricles and the subarachnoid space. It acts as a cushion, absorbing shock and protecting delicate neural tissue from injury. CSF also helps maintain stable pressure within the skull, removes metabolic waste, transports nutrients and hormones, and provides buoyancy—reducing the effective weight of the brain so it doesn’t compress its own blood vessels or nerves. Produced by the choroid plexus and reabsorbed into the bloodstream through arachnoid granulations, CSF continuously circulates in a controlled cycle essential for normal nervous system function.
Blood–Brain Barrier (BBB)
The blood–brain barrier is a highly selective protective barrier that separates the brain’s delicate neural tissue from the circulating blood. It is formed by tightly packed endothelial cells lining the brain’s capillaries, supported by astrocytes and a specialised basement membrane. These structures limit what can pass from the bloodstream into the brain, allowing essential substances such as oxygen, glucose, and certain amino acids to enter while blocking toxins, pathogens, and many medications. This strict filtering system helps maintain a stable chemical environment necessary for proper neuronal function, protects against harmful fluctuations in blood composition, and prevents inflammation and infection within the central nervous system.
What can cross the Blood-Brain Barrer:
Small, lipid-soluble molecules → e.g., oxygen, carbon dioxide, alcohol, some anesthetics
Essential nutrients via transporters → e.g., glucose (via GLUT1), amino acids
Some medications only if lipid-soluble or designed to cross
What cannot cross the Blood-Brain Barrer:
Most large molecules, proteins, and charged substances
Many common drugs, including most antibiotics and chemotherapy agents
Pathogens — which is why CNS infections are less common but more dangerous
Microglia
Microglia are the resident immune cells of the central nervous system and act as the brain’s main line of defence. They constantly monitor the neural environment for signs of infection, injury, or abnormal activity, and respond by removing pathogens, clearing debris, and engulfing damaged or dead cells through phagocytosis. Beyond immune protection, microglia also help maintain healthy neural function by pruning unnecessary synapses during development, releasing signalling molecules that regulate inflammation, and supporting tissue repair after injury. Their activity must remain tightly controlled—overactivation can contribute to neuroinflammatory conditions, while impaired microglial function can lead to inadequate protection and poor neural health.
Clinical Connections
Given the diverse roles of the nervous system, pathology in this body system produces a wide spectrum of clinical signs and symptoms, each reflecting the underlying area of dysfunction. The following examples illustrate how neurological disorders may present in practice:
Cerebral Lobes and Localised Brain Injury
Damage to specific brain regions leads to predictable clinical changes because each lobe has specialised functions. For example, injury to the frontal lobe—often seen in trauma, tumours, or stroke—can cause impaired judgement, personality changes, reduced impulse control, and difficulty planning or initiating movements. Patients may appear disinhibited, emotionally flat, or unable to concentrate.
In contrast, occipital lobe damage can lead to visual disturbances, while temporal lobe injury may affect memory and language comprehension. Understanding these functional areas helps clinicians quickly recognise the location and likely cause of neurological deficits.
Cerebrospinal Fluid (CSF) Disorders
The production, flow, or absorption of CSF can be disrupted by conditions such as hydrocephalus, meningitis, or subarachnoid haemorrhage. Elevated CSF pressure may cause headache, vomiting, papilledema, or altered consciousness due to compression of brain tissue. In meningitis, inflammation of the meninges can impair CSF circulation and compromise the blood–brain barrier, allowing toxins and pathogens to enter neural tissue. Recognising CSF-related symptoms is crucial because early intervention can prevent permanent neurological damage.
Vascular System: Stroke and Perfusion Problems
The brain depends on a constant and uninterrupted blood supply, so vascular disruption has immediate consequences. In an ischaemic stroke, a blocked artery deprives brain tissue of oxygen, leading to sudden weakness, slurred speech, vision loss, or facial droop—symptoms that reflect the region affected. A haemorrhagic stroke, caused by bleeding into or around the brain, can rapidly increase intracranial pressure and cause severe headache, vomiting, or rapid deterioration. Quick identification of stroke patterns allows clinicians to determine which part of the nervous system is compromised and guides appropriate emergency treatment.
Peripheral Nervous System and Nerve Damage
Damage to peripheral nerves—through compression, trauma, diabetes, or autoimmune conditions—produces clinical signs tied to the sensory or motor pathways involved. For example, carpal tunnel syndrome affects the median nerve, causing numbness, tingling, and weakness in the hand. Peripheral neuropathy from diabetes leads to sensory loss in the feet, increasing risk of injury and infection. Because the PNS follows predictable anatomical pathways, clinicians can often identify the exact nerve affected simply by mapping the patient’s symptoms.
Concept Check
1. A patient presents with severe headache, vomiting, and papilledema. What does this suggest about their CSF dynamics, and what conditions could cause this?
2. Certain antibiotics effectively treat lung infections but fail to improve bacterial meningitis. Explain how the blood–brain barrier influences treatment choices in this case.
3. A patient with multiple sclerosis reports numbness and delayed limb movement. How does demyelination explain these symptoms?
4. A patient suddenly develops weakness on one side of the body and slurred speech. What type of neurological event is most likely occurring, and which structures are probably involved?
5. If a drug increases inhibitory neurotransmission, what effect might this have on neural activity and the patient’s behaviour or consciousness? Explain your reasoning.