Pyelonephritis: Upper Urinary Tract Infection and Renal Parenchymal Inflammation
Pyelonephritis is an infection of the renal pelvis and kidney parenchyma that results in inflammation, tissue injury, and impaired renal function. Unlike lower urinary tract infection, pyelonephritis directly involves the kidney, placing patients at risk of acute kidney injury and systemic illness.
What You Need to Know
Pyelonephritis is a bacterial infection of the renal parenchyma and collecting system that occurs when pathogens ascend from the lower urinary tract or, less commonly, spread through the bloodstream. Unlike simple cystitis, which is confined to the bladder, pyelonephritis involves the kidney itself, making it a potentially life-threatening condition due to the risk of sepsis and permanent renal damage.
The kidneys are highly vascular and metabolically active, so infection within renal tissue triggers a strong inflammatory response. This leads to interstitial oedema, tubular dysfunction, and impaired urine concentration and filtration. As inflammation increases, renal blood flow and filtration can be reduced, contributing to acute kidney injury during severe or untreated infection.
Pyelonephritis most commonly develops when bacteria are able to bypass or overwhelm normal urinary tract defences. This risk is increased by:
urinary obstruction or reflux
indwelling catheters or instrumentation
pregnancy
diabetes or immunosuppression
Because the kidneys are responsible for filtering the blood, infection within renal tissue also creates a direct pathway for bacteria and inflammatory mediators to enter the systemic circulation. This explains why pyelonephritis frequently presents with fever, flank pain, and systemic illness rather than isolated urinary symptoms, and why prompt recognition and treatment are essential to prevent sepsis and long-term renal injury.
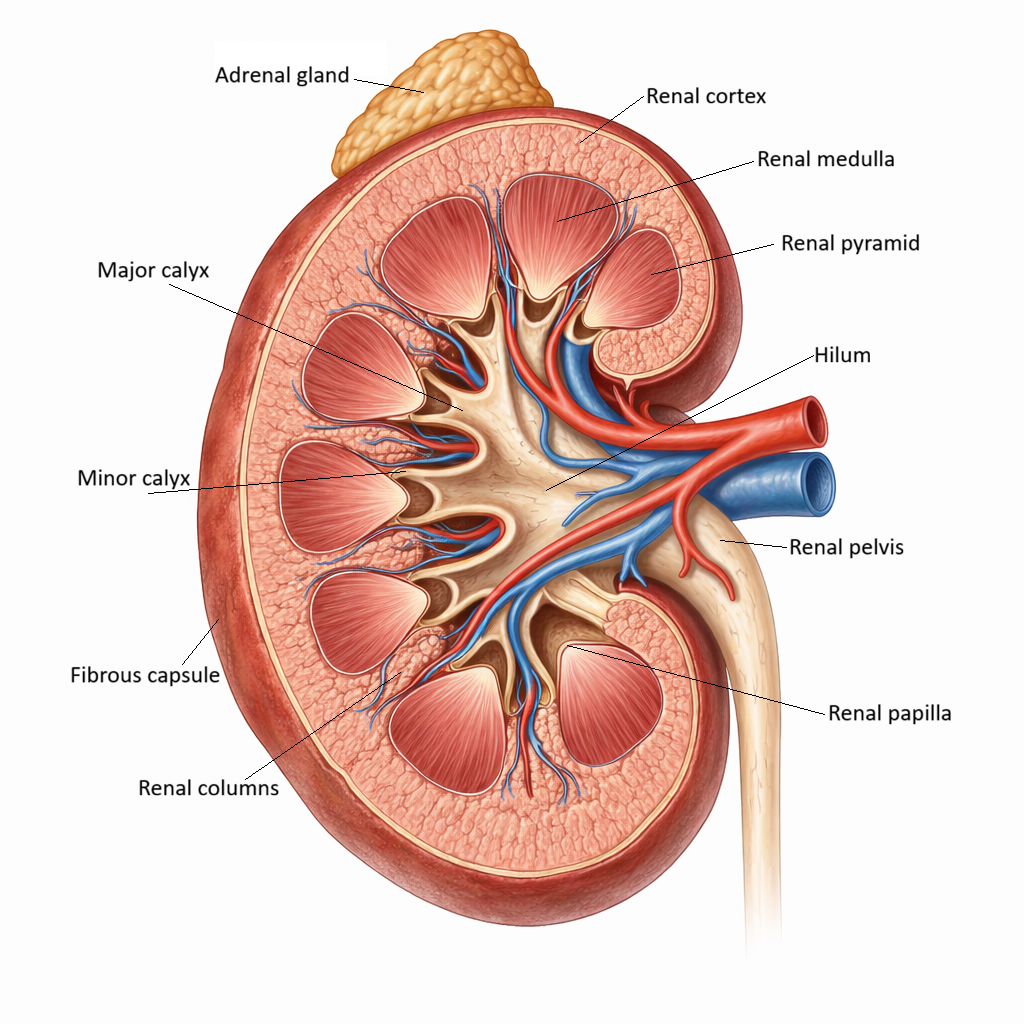
Image: The kidney consists of the cortex, medulla, and collecting system, which work together to filter blood and produce urine. In pyelonephritis, bacterial infection ascends to involve the renal parenchyma and pelvis, causing inflammation that can impair function and, in severe cases, lead to scarring.
Beyond the Basics
Ascending infection and renal invasion
Most cases of pyelonephritis arise from ascending infection rather than haematogenous spread. Bacteria that colonise the bladder are able to migrate upward through the ureters when normal urinary flow is impaired by stasis, reflux, obstruction, or instrumentation. Uropathogens such as E. coli are particularly well adapted for this process because they possess fimbriae and adhesion molecules that allow them to bind tightly to uroepithelial surfaces and resist being flushed away by urine. As organisms ascend into the renal pelvis and calyces, they encounter an environment that is no longer just a conduit for urine but a highly vascularised organ with direct access to the bloodstream.
Once bacteria reach the kidney, they are able to enter the renal parenchyma through the collecting ducts and adhere directly to tubular epithelial cells. From there they penetrate into the interstitium, establishing infection within the tissue itself rather than remaining confined to the urinary space. This step marks the transition from lower urinary tract infection to pyelonephritis and explains why the disease is associated with systemic inflammation, flank pain, and the risk of bacteraemia. At this point the kidney is not just hosting bacteria, it is actively being injured by their presence.
Inflammatory response and tubular dysfunction
The arrival of bacteria within renal tissue activates a powerful innate immune response. Neutrophils, macrophages, and inflammatory mediators are recruited into the interstitium and around the tubules in an attempt to contain and destroy the infection. While this response is necessary for pathogen clearance, it also damages the surrounding renal cells. Cytokines, proteolytic enzymes, and reactive oxygen species disrupt epithelial membranes and impair the transport proteins that normally regulate sodium, water, and solute movement across the tubular wall.
As tubular cells become inflamed and injured, their ability to concentrate urine and reclaim electrolytes declines. Sodium and water are lost inappropriately into the urine, contributing to polyuria, dehydration, and electrolyte disturbance even while the patient is systemically unwell. This functional tubular failure is a key reason why pyelonephritis often produces abnormalities in fluid balance and blood chemistry that extend beyond what would be expected from fever or reduced intake alone.
Renal oedema, hypoxia, and acute kidney injury
Inflammation within the kidney increases capillary permeability, allowing fluid and plasma proteins to leak into the interstitial space and produce renal oedema. Unlike many other organs, the kidney is enclosed by a relatively rigid capsule that limits its ability to expand. As tissue swells, intrarenal pressure rises and small blood vessels become compressed, reducing oxygen delivery to already stressed tubular cells. This creates a secondary ischaemic injury superimposed on the infectious damage.
Tubular cells are particularly vulnerable to hypoxia because they require large amounts of ATP to drive active transport processes. When oxygen delivery falls, energy production drops and cells lose their ability to maintain membrane gradients, further worsening tubular dysfunction. This is why pyelonephritis can precipitate acute kidney injury even when the infection is treated promptly and why recovery of renal function may lag behind resolution of fever and bacteraemia.
Systemic spread and sepsis physiology
The kidneys receive a large fraction of the cardiac output, which makes them highly efficient at filtering blood but also creates a direct route for bacteria and inflammatory mediators to enter the circulation once renal tissue is infected. Disruption of capillary integrity allows organisms and cytokines to escape into the bloodstream, producing bacteraemia and triggering a systemic inflammatory response. This systemic reaction leads to widespread vasodilation, capillary leak, and microvascular dysfunction.
These haemodynamic changes reduce effective renal perfusion even further, amplifying the original kidney injury. As blood pressure falls and microcirculatory flow becomes erratic, oxygen delivery to the kidneys and other organs declines, creating a vicious cycle in which infection, inflammation, and hypoperfusion reinforce one another. This is the physiological basis of septic shock arising from pyelonephritis.
Acute and chronic patterns of injury
When pyelonephritis is treated promptly, inflammation can resolve and tubular cells are often able to recover, allowing renal function to return close to baseline. However, when infection is recurrent or persistent — particularly in the presence of reflux, obstruction, or structural abnormality — each episode leaves behind microscopic areas of scarring. Over time these scars accumulate, leading to tubular atrophy, interstitial fibrosis, and progressive nephron loss.
Chronic pyelonephritis therefore represents not a single infection but the cumulative result of repeated inflammatory injury. The resulting architectural distortion of the kidney contributes to long-term declines in filtration, impaired urine concentration, and the development of secondary hypertension.
Clinical Connections
Pyelonephritis typically presents with fever, rigors, flank or costovertebral angle tenderness, nausea, vomiting, and dysuria or urinary frequency, but older adults and immunocompromised patients may present atypically with delirium, falls, or general functional decline rather than classic urinary symptoms. Because the infection involves renal tissue rather than just the bladder, patients often appear systemically unwell, with tachycardia, hypotension, and signs of sepsis developing early in the course of illness.
At the bedside, clinicians commonly see:
fever with raised inflammatory markers and positive urine culture
loin tenderness or flank pain on examination
reduced urine output or rising creatinine due to tubular dysfunction and hypoperfusion
hypotension or altered mental state when bacteraemia or sepsis is present
Management requires prompt intravenous antibiotics that achieve adequate renal tissue penetration, along with careful fluid resuscitation to support renal perfusion and correct dehydration. Imaging is often required to identify obstruction, stones, or reflux, as these prevent eradication of infection and allow recurrent or persistent pyelonephritis. Failure to correct underlying structural or functional abnormalities increases the risk of acute kidney injury, renal scarring, and progression to chronic kidney disease.
Concept Check
Why does pyelonephritis cause more severe illness than lower urinary tract infection?
How does renal inflammation impair tubular function and urine concentration?
Why can pyelonephritis precipitate acute kidney injury?
How does renal vascularity increase the risk of sepsis?
Why does recurrent pyelonephritis lead to chronic kidney damage?