Renal System - OVerview
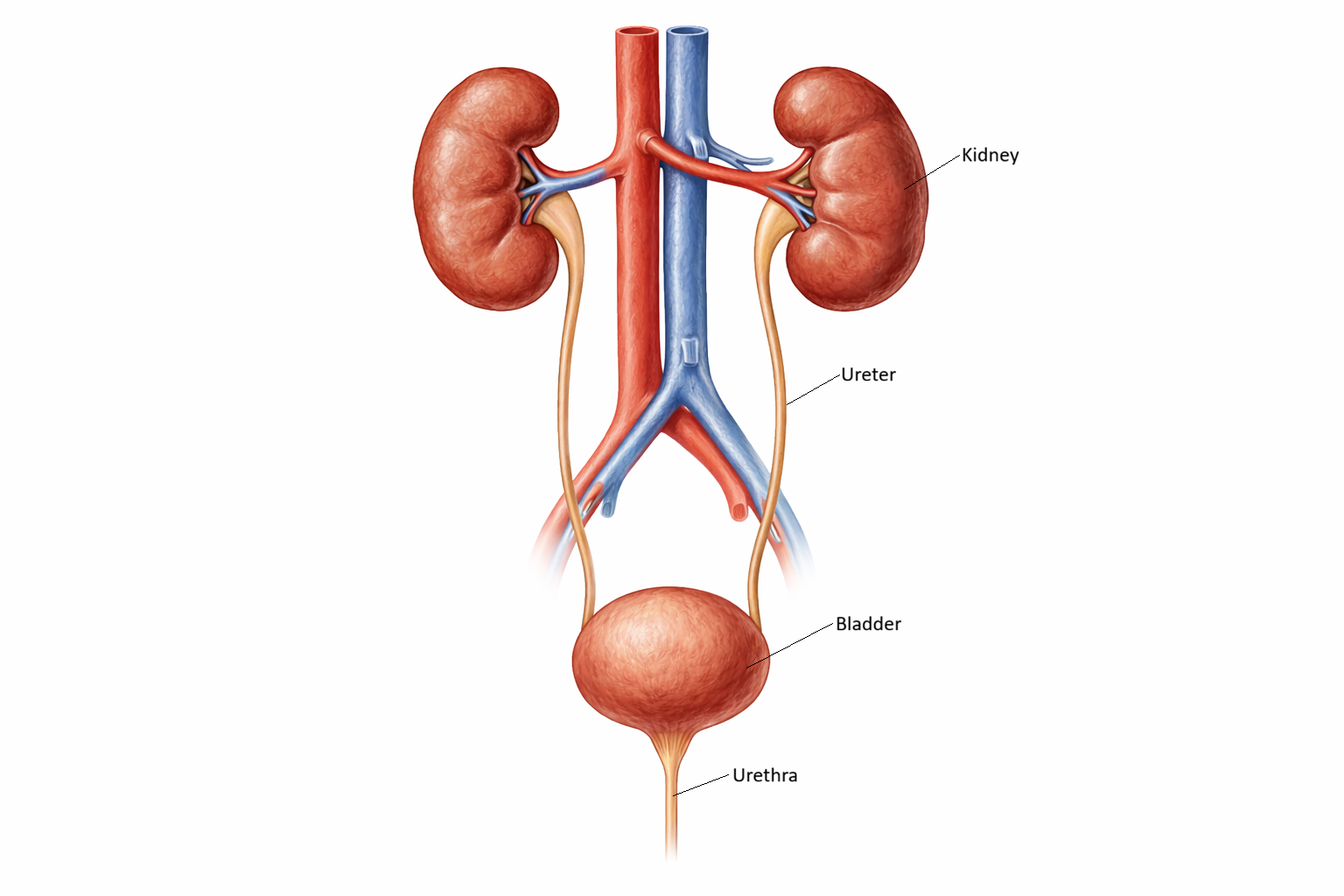
The renal (urinary) system plays a crucial role in maintaining the body’s internal balance by regulating fluid volume, electrolyte concentrations, acid–base status, and the removal of metabolic waste products. It consists primarily of the kidneys, ureters, bladder, and urethra, which work together to filter the blood, produce urine, store it, and eliminate it from the body. Beyond waste removal, the kidneys function as major endocrine organs, producing hormones that regulate blood pressure, stimulate red blood cell production, and activate vitamin D. As a result, even mild dysfunction can have widespread systemic effects. For nurses, understanding renal physiology is essential for managing fluid balance, recognising early signs of kidney injury, interpreting laboratory results, administering nephrotoxic medications safely, and caring for patients with chronic kidney disease, dehydration, infections, or electrolyte disturbances.
What You Need to Know
The renal system is responsible for maintaining the chemical and fluid stability of the body. Its primary organs, the kidneys, are highly vascular, bean-shaped structures located in the retroperitoneum on either side of the spine. Each kidney contains more than one million nephrons, which act as microscopic processing units that filter the blood, remove waste, and precisely regulate water and electrolyte balance. Blood enters the kidneys through the renal arteries and flows through progressively smaller vessels until it reaches the glomerulus, a specialised capillary network where filtration begins. At this site, water and small solutes pass into the nephron while blood cells and large proteins remain in the circulation.
Once filtered, fluid moves through the nephron’s tubular system, where its composition is continuously adjusted. The proximal tubule reabsorbs most of the filtered water, electrolytes, glucose, and amino acids, returning these vital substances to the bloodstream. The loop of Henle establishes a concentration gradient in the renal medulla, which later allows the kidneys to conserve or excrete water as needed. The distal tubule and collecting ducts then fine-tune sodium, potassium, acid–base balance, and water content under the influence of key hormones.
As filtrate passes through the nephron, different segments make distinct contributions:
the glomerulus filters plasma into tubular fluid
the proximal tubule performs bulk reabsorption of water and solutes
the loop of Henle creates the medullary gradient for urine concentration
the distal tubule and collecting ducts adjust electrolytes, acid–base status, and water balance
Together, these processes transform plasma into urine while preserving the stability of the internal environment.
Once urine has been formed, it drains from the kidneys into the ureters, which are muscular tubes that propel urine toward the bladder through rhythmic peristaltic contractions. The bladder acts as a temporary storage reservoir, expanding as it fills and activating stretch receptors that signal the need to void. Urination occurs when the detrusor muscle contracts and the urethral sphincters relax in a coordinated, neurologically controlled process. Because this coordination depends on intact nerve pathways, normal urinary function is closely linked to nervous system health as well as kidney function.
Beyond the Basics
Acid–Base Regulation: Long-Term pH Control
Beyond producing urine, the kidneys are the body’s primary regulators of long-term acid–base balance. Every day, normal metabolism generates non-volatile acids that cannot be eliminated by the lungs and must be excreted by the kidneys. This is achieved by secreting hydrogen ions into the urine while simultaneously reabsorbing or generating bicarbonate, the body’s main buffering base.
When metabolic acidosis develops, the kidneys increase hydrogen ion secretion and produce new bicarbonate to raise blood pH. In metabolic alkalosis, they reduce hydrogen ion secretion and allow bicarbonate to be lost in the urine. This slow but powerful regulation stabilises pH in a way that the lungs alone cannot achieve.
Blood Pressure Control: The Renin–Angiotensin–Aldosterone System
The kidneys act as pressure sensors for the circulatory system. When renal blood flow falls — due to dehydration, haemorrhage, or heart failure — specialised juxtaglomerular cells release renin. Renin initiates the renin–angiotensin–aldosterone system (RAAS), which increases vascular tone and promotes sodium and water retention.
Through this system, the kidneys directly influence:
blood volume
arterial pressure
renal perfusion
Chronic over-activation of RAAS contributes to hypertension, heart failure, and progressive kidney disease, highlighting the kidney’s central role in cardiovascular regulation.
Endocrine Functions: Erythropoietin and Vitamin D
The kidneys also function as endocrine organs. They produce erythropoietin (EPO) in response to tissue hypoxia. EPO stimulates red blood cell production in the bone marrow, ensuring adequate oxygen delivery to tissues. In chronic kidney disease, reduced EPO production leads to anaemia, contributing to fatigue, reduced exercise tolerance, and cardiovascular strain.
The kidneys are also responsible for converting vitamin D into its active form, calcitriol. Calcitriol increases intestinal calcium absorption and regulates bone metabolism. When kidney function declines, this activation step is impaired, leading to low calcium levels, secondary hyperparathyroidism, and progressive bone demineralisation.
Glomerular Filtration Rate (GFR): Measuring Renal Performance
Glomerular filtration rate (GFR) provides an overall indication of kidney function. It indicates how much plasma is filtered by the glomeruli each minute and therefore how effectively the kidneys can remove waste and regulate fluid and electrolytes.
GFR falls with:
ageing
dehydration
shock
acute kidney injury
chronic kidney disease
Clinically, GFR is used to stage kidney disease, guide drug dosing, and assess the urgency of intervention. Even small reductions in GFR can significantly alter drug clearance and electrolyte balance.
Electrolyte Regulation: Maintaining Electrical and Chemical Stability
The kidneys tightly regulate plasma concentrations of sodium, potassium, chloride, magnesium, calcium, and phosphate. These electrolytes determine:
fluid distribution
nerve conduction
muscle contraction
cardiac rhythm
Because renal handling of electrolytes depends on precise tubular transport, even mild kidney dysfunction can produce dangerous disturbances such as hyperkalaemia, hyponatraemia, or acidosis. This explains why kidney disease so often presents with cardiovascular, neurological, and muscular complications.
Clinical Connections
Renal and urinary disorders are among the most common conditions encountered in clinical practice and can progress rapidly if not recognised early. Acute kidney injury (AKI) often develops in response to dehydration, sepsis, hypovolaemia, obstruction, or exposure to nephrotoxic medications such as NSAIDs, contrast agents, and some antibiotics. Early changes in urine output, rising creatinine, fluid retention, and electrolyte abnormalities such as hyperkalaemia are often the first indicators. Because AKI is frequently reversible in its early stages, prompt identification and correction of the underlying cause is critical to prevent permanent nephron loss.
Chronic kidney disease (CKD) evolves more slowly and is most commonly driven by diabetes, hypertension, and autoimmune disease. As nephron function declines, patients develop characteristic complications including anaemia from reduced erythropoietin production, fluid overload from impaired sodium and water excretion, bone disease from disordered vitamin D and calcium metabolism, and progressive accumulation of metabolic toxins. Recognising these patterns allows clinicians to stage disease, adjust medications, and initiate protective therapies before irreversible failure occurs.
Urinary tract infections present with distinct patterns depending on the level of infection. Lower tract infections (cystitis) cause dysuria, urgency, frequency, and cloudy or malodorous urine, while upper tract infections (pyelonephritis) produce flank pain, fever, rigors, and systemic illness. In older adults, infection may present primarily with delirium or functional decline rather than urinary symptoms, making vigilance essential.
Urinary obstruction, whether due to prostatic enlargement, strictures, tumours, or stones, can silently impair renal drainage. Persistent back-pressure leads to hydronephrosis and progressive kidney injury even when pain is minimal. Renal calculi produce intense colicky flank pain and haematuria when they obstruct urine flow, and they increase the risk of infection and long-term renal damage.
Incontinence reflects disruption of neural, muscular, or sphincter control and can arise from neurological disease, pelvic floor dysfunction, medications, or urinary retention. It has major physical and psychological consequences and requires careful, non-judgmental assessment.
Because the kidneys regulate fluid and electrolyte balance, disturbances such as dehydration or fluid overload quickly manifest as changes in blood pressure, weight, urine output, and laboratory values. Continuous monitoring of intake and output, daily weights, and electrolytes is therefore fundamental to detecting renal deterioration and guiding safe clinical care.
Concept Check
Describe how the nephron filters blood, modifies the filtrate, and ultimately produces urine. Which sections of the nephron are responsible for each function?
How does the renin–angiotensin–aldosterone system help regulate blood pressure and fluid balance? Why is this system clinically important?
Explain how the kidneys maintain acid–base balance and what happens when this function is impaired.
Why do patients with chronic kidney disease often develop anaemia, bone disorders, and electrolyte imbalances?
A patient presents with flank pain, fever, nausea, and painful urination. Which renal condition might this indicate, and what complications should you monitor for?