PENILE ANATOMY & PHYSIOLOGY
The penis is a highly specialised organ responsible for sexual function, urination and delivery of sperm into the female reproductive tract. Its structure integrates vascular, muscular, connective tissue and neural components that together enable erection, penetration and ejaculation. Erection is a neurovascular event driven by parasympathetic activity and changes in blood flow, while ejaculation is a coordinated sequence involving sympathetic, somatic and spinal reflex pathways. Understanding penile anatomy and physiology is essential for interpreting erectile function, sexual health, male fertility and the mechanisms underlying erectile dysfunction.
What You Need to Know
The penis is a specialised external organ designed for both urinary excretion and sexual function. Its structure is built around three columns of erectile tissue: the paired corpora cavernosa, which provide rigidity during erection, and the corpus spongiosum, which surrounds the urethra and expands to form the glans penis. This arrangement allows the penis to become firm enough for penetration while keeping the urethral lumen patent for semen delivery during ejaculation.
Erection is a vascular event tightly regulated by neural input and local chemical signalling. Sexual stimulation activates parasympathetic pathways that trigger release of nitric oxide within penile tissue, leading to smooth muscle relaxation, arterial dilation, and increased blood flow into the erectile spaces. As the corpora cavernosa fill, venous outflow is compressed, trapping blood and producing rigidity.
The corpus spongiosum also engorges but to a lesser degree, preventing urethral compression and ensuring semen can pass freely. Key functional elements involved in erection include:
Nitric oxide–mediated vasodilation, allowing increased arterial inflow
Relaxation of cavernosal smooth muscle, enabling expansion of erectile tissue
Venous compression, maintaining rigidity by limiting blood outflow
Ejaculation is a distinct process that follows erection and is controlled by separate neural pathways. It occurs in two coordinated phases. Emission involves sympathetic-mediated movement of sperm and glandular secretions into the prostatic urethra, while expulsion relies on rhythmic contraction of pelvic floor and perineal muscles to propel semen through the urethra and out of the body. Sensory input from the glans penis, which contains a high density of tactile and pressure receptors, plays a central role in initiating and sustaining sexual arousal. Penile anatomy, vascular dynamics, and neural control ensure effective erection, ejaculation, and delivery of semen during intercourse.
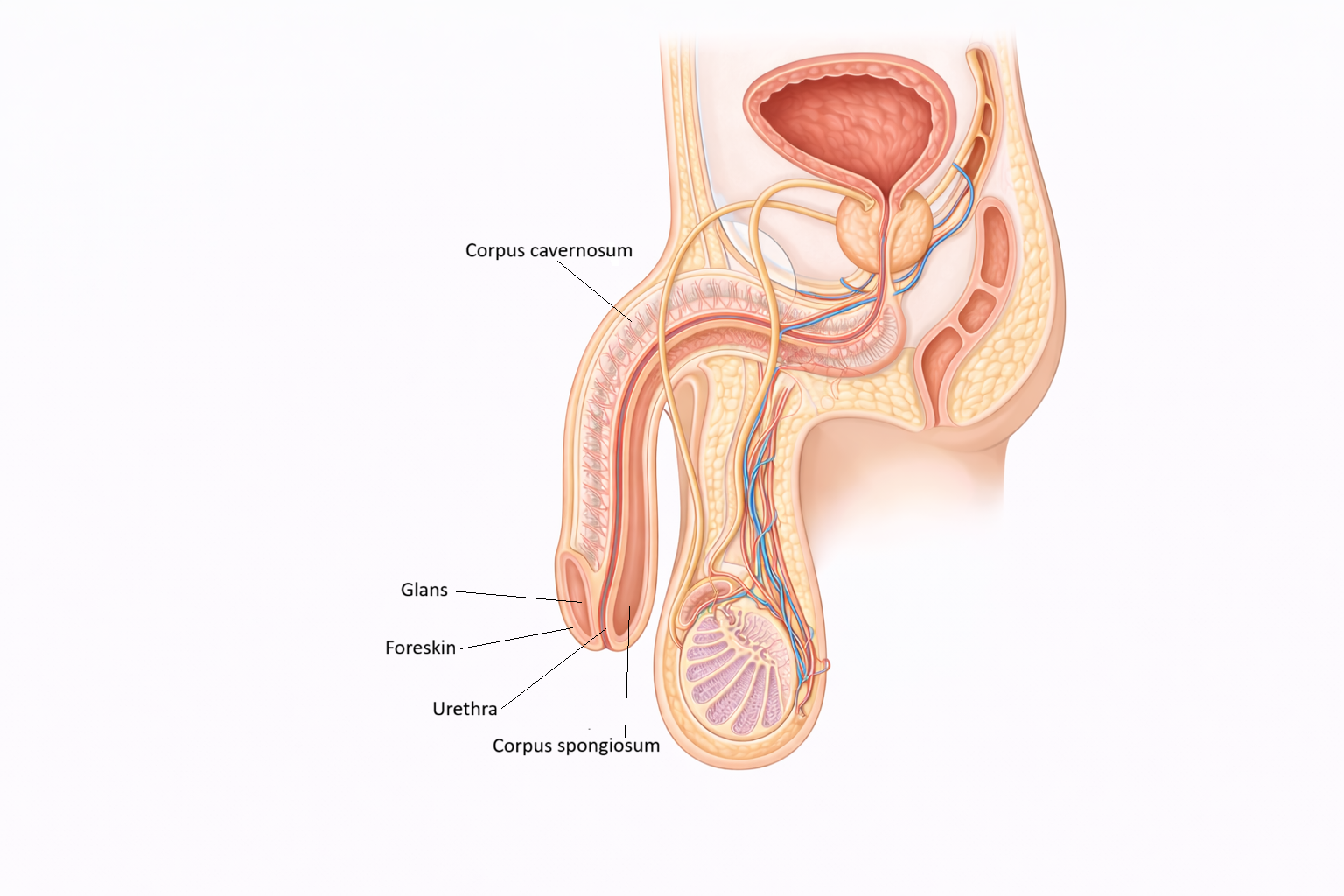
Image: The penis contains two corpora cavernosa and a single corpus spongiosum, which surrounds the urethra and expands distally to form the glans. These erectile tissues become engorged with blood during arousal, allowing for rigidity while maintaining a patent urethra for the passage of semen and urine.
Beyond the Basics
Anatomical Structure of Erectile Tissue
The penis contains three columns of erectile tissue that differ in structure and mechanical function. The paired corpora cavernosa lie dorsally and are composed of interconnected vascular spaces known as sinusoids, lined by endothelium and surrounded by smooth muscle. These spaces are enclosed by the tunica albuginea, a dense fibrous sheath that is critical for generating rigidity during erection. The tunica albuginea has a layered architecture that limits expansion outward and instead promotes pressure build-up within the erectile tissue.
The corpus spongiosum lies ventrally and surrounds the urethra. Although it also contains erectile tissue, it remains more compliant during erection, preventing compression of the urethra and allowing uninterrupted passage of semen. Distally, the corpus spongiosum expands to form the glans penis, which contains a high density of sensory receptors and plays a key role in sexual stimulation and reflex activation.
Blood Supply and Venous Occlusion
Arterial supply to the penis arises from branches of the internal pudendal artery, particularly the cavernous arteries that run centrally through each corpus cavernosum. In the flaccid state, these arteries are relatively constricted, and blood flow through the sinusoids is limited.
During sexual arousal, smooth muscle relaxation allows the cavernous arteries to dilate, rapidly increasing arterial inflow. As the sinusoids fill and expand, they compress the subtunical venules against the tunica albuginea. This compression markedly reduces venous outflow, a process known as the veno-occlusive mechanism. Maintenance of erection depends on this balance between sustained inflow and restricted outflow. When arousal subsides, smooth muscle contraction restores venous drainage, returning the penis to its flaccid state.
Neural Control of Erection
Erection is primarily mediated by parasympathetic fibres originating from the sacral spinal cord segments S2 to S4. Sexual stimulation, whether tactile or psychogenic, activates these pathways and triggers release of nitric oxide from endothelial cells and non-adrenergic, non-cholinergic nerve terminals within the erectile tissue.
Nitric oxide stimulates production of cyclic GMP within smooth muscle cells, leading to smooth muscle relaxation, arterial dilation, and increased blood filling of the sinusoids. Cyclic GMP is degraded by phosphodiesterase type 5, and inhibition of this enzyme prolongs smooth muscle relaxation. This mechanism forms the basis of phosphodiesterase-5 inhibitor medications used in erectile dysfunction.
Somatic and Sensory Contributions
Somatic innervation of the penis is supplied by the pudendal nerve. Sensory branches, including the dorsal nerve of the penis, transmit tactile and pressure information from the glans, foreskin, and shaft to the central nervous system. This sensory input reinforces arousal and contributes to the coordination of ejaculation.
Motor branches of the pudendal nerve innervate the bulbospongiosus and ischiocavernosus muscles. Contraction of these muscles increases intracavernosal pressure, enhances penile rigidity, and plays a key role in semen expulsion during ejaculation.
Ejaculation: Emission and Expulsion
Ejaculation is a coordinated reflex consisting of two distinct but sequential phases. During the emission phase, sympathetic fibres originating from spinal segments T12 to L2 stimulate contraction of the epididymis, vas deferens, seminal vesicles, and prostate. This propels sperm and glandular secretions into the prostatic urethra. Simultaneous contraction of the internal urethral sphincter prevents semen from entering the bladder.
The expulsion phase follows and is mediated by somatic motor pathways. Rhythmic contraction of the bulbospongiosus and pelvic floor muscles generates pulsatile increases in urethral pressure, forcing semen through the urethra and out of the body. This phase is accompanied by intense sensory feedback and tightly coordinated autonomic activity.
Refractory Period and Recovery
After ejaculation, a refractory period occurs during which erection and ejaculation are temporarily suppressed. This phase is associated with increased sympathetic tone and central neurochemical changes that reduce sexual responsiveness. The duration of the refractory period varies with age, hormonal status, and individual physiology, reflecting the integrated control of sexual function by vascular, neural, and endocrine systems.
Clinical Connections
Penile function depends on intact vascular supply, neural signalling, smooth muscle responsiveness, and hormonal support. Erectile dysfunction can arise when any of these components are disrupted, which is why ED is often an early indicator of broader systemic disease rather than an isolated genital problem. Vascular pathology, particularly endothelial dysfunction associated with diabetes, hypertension, or atherosclerosis, impairs nitric oxide signalling and reduces arterial inflow to erectile tissue. Neurological injury, hormonal imbalance, psychological stressors, and medication effects may further interfere with erection by altering neural input or smooth muscle tone.
Several common clinical conditions affecting erection and ejaculation can be understood by linking symptoms back to underlying anatomy and physiology:
Erectile dysfunction, resulting from impaired nitric oxide signalling, reduced arterial inflow, or failure of the veno-occlusive mechanism
Peyronie’s disease, where fibrous plaque formation within the tunica albuginea restricts uniform expansion of the corpora cavernosa and causes curvature or pain
Ejaculatory disorders, including premature ejaculation, anejaculation, and retrograde ejaculation due to autonomic or somatic nerve dysfunction
Priapism, a prolonged erection caused by failure of venous outflow, leading to ischemia within the corpora cavernosa
Understanding nitric oxide–cGMP signalling and venous occlusion explains the effectiveness of phosphodiesterase-5 inhibitors, which prolong smooth muscle relaxation and support erection in the presence of intact neural and vascular input. Conversely, conditions such as Peyronie’s disease highlight the mechanical importance of the tunica albuginea in maintaining rigidity and symmetry during erection.
Disorders of ejaculation often reflect disruption of neural coordination rather than erectile failure. Diabetes, spinal cord injury, pelvic surgery, or medications affecting sympathetic tone can interfere with emission, expulsion, or bladder neck closure. Retrograde ejaculation occurs when the internal urethral sphincter fails to contract, allowing semen to enter the bladder rather than exit the urethra.
Priapism represents a urological emergency. Prolonged trapping of deoxygenated blood within the corpora cavernosa leads to tissue hypoxia, acidosis, and risk of permanent erectile damage if not promptly treated. Recognising priapism as a failure of detumescence rather than excessive arousal is essential for timely intervention and preservation of erectile function.
Concept Check
What structural features of the corpora cavernosa enable rigidity during erection?
How does nitric oxide mediate erection, and why is PDE5 important in this process?
Distinguish between the emission and expulsion phases of ejaculation.
How does venous occlusion maintain an erection?
What neural pathways regulate erection versus ejaculation?