PNEUMOTHORAX: Loss of Negative Intrapleural Pressure Leading to Lung Collapse
Pneumothorax occurs when air enters the pleural space, disrupting the negative pressure that normally keeps the lung expanded against the chest wall. As intrapleural pressure rises toward atmospheric pressure, the affected lung partially or completely collapses. This loss of lung expansion impairs ventilation and reduces effective gas exchange. A Pneumothorax can arise spontaneously, as a result of trauma, or as a complication of underlying lung disease or medical intervention. The physiological consequences depend on the volume of air in the pleural space, the speed of accumulation and whether the pressure continues to rise with each breath.
What You Need to Know
A pneumothorax occurs when air enters the pleural space, disrupting the normal negative intrapleural pressure that keeps the lungs expanded. Under physiological conditions, the pleural cavity maintains a pressure lower than atmospheric pressure, counteracting the natural elastic recoil of lung tissue. This pressure gradient allows the lungs to remain inflated throughout the respiratory cycle. When air leaks into the pleural space, the pressure equalises with or exceeds atmospheric pressure, removing the force that holds the lung open.
Loss of negative intrapleural pressure allows the affected lung to partially or completely collapse. As lung volume decreases, ventilation to that region falls sharply. Blood flow may continue through the collapsed or poorly ventilated alveoli, creating ventilation–perfusion mismatch and reducing arterial oxygen levels. Hypoxaemia develops in proportion to the size of the pneumothorax and the amount of lung excluded from ventilation.
Physiological consequences of pneumothorax include:
Reduced lung expansion, due to unopposed elastic recoil
Ventilation–perfusion mismatch, as perfusion persists despite impaired ventilation
Increased work of breathing, particularly when lung volume is significantly reduced
The clinical impact varies widely. Small, stable pneumothoraces may produce minimal symptoms and limited physiological disturbance, especially in individuals with healthy lungs. Larger or progressive pneumothoraces cause more significant lung collapse, rapid deterioration in gas exchange, and escalating respiratory distress. The speed at which air enters the pleural space is critical, as rapid accumulation increases the risk of severe hypoxaemia and cardiorespiratory compromise.
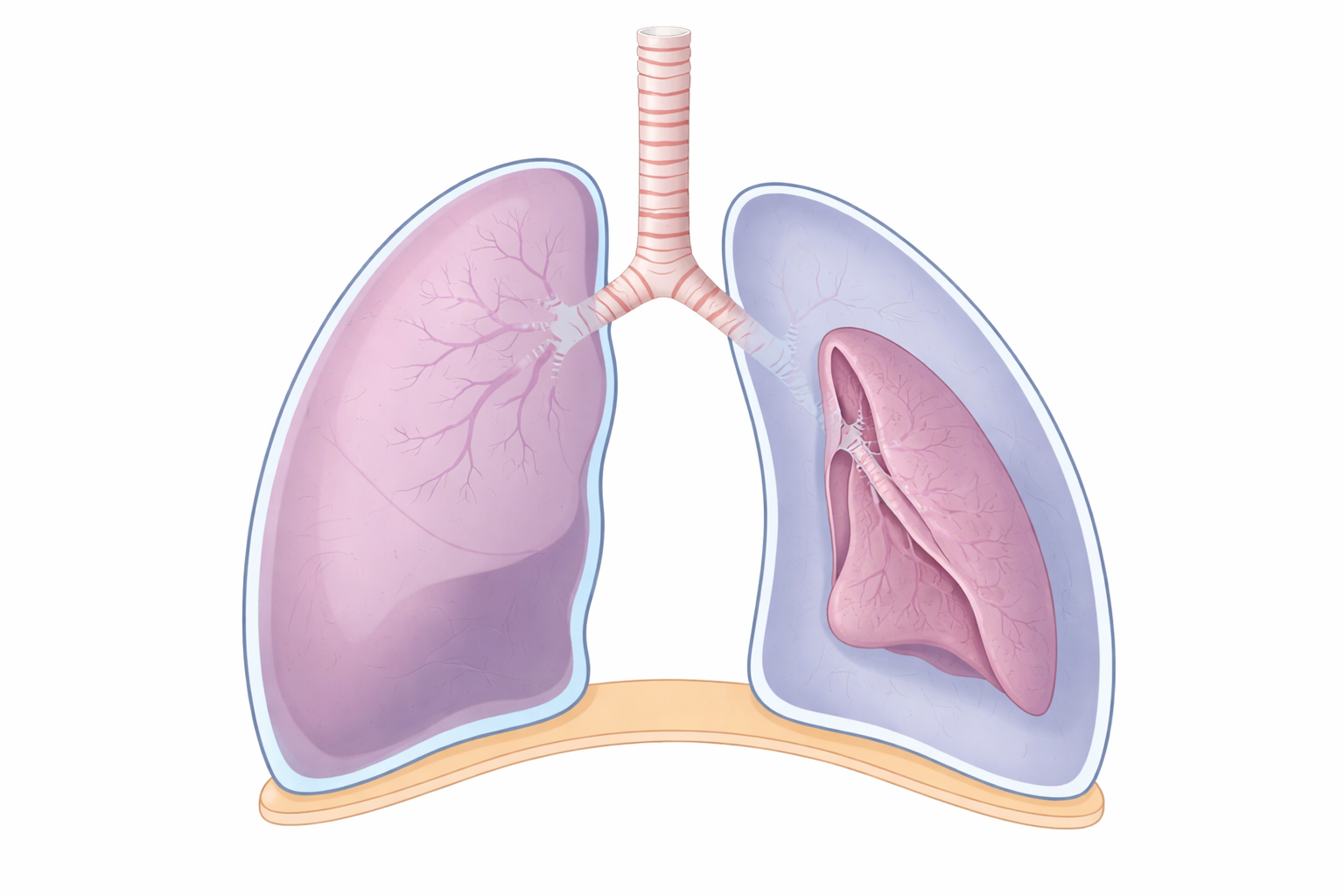
Image: The right lung (pn the left side of the image) remains fully expanded, while the other has collapsed inward due to air in the pleural space, separating the lung from the chest wall and preventing normal expansion.
Beyond the Basics
Mechanisms of Air Entry Into the Pleural Space
Air enters the pleural space when the integrity of the lung surface or chest wall is disrupted, allowing atmospheric air or alveolar gas to leak into a space that is normally sealed. In spontaneous pneumothorax, rupture of small subpleural blebs allows air to escape directly from the lung into the pleural cavity. This can occur in people without known lung disease, often due to focal weaknesses at the lung apex, or in those with underlying pathology that compromises alveolar structure.
Secondary pneumothorax arises when structurally abnormal lung tissue ruptures. Conditions such as chronic obstructive pulmonary disease, cystic fibrosis, and interstitial lung disease weaken alveolar walls, making them prone to rupture even with modest increases in intrathoracic pressure. Traumatic pneumothorax occurs following blunt or penetrating chest injury, where air enters through a chest wall defect or damaged lung. Iatrogenic pneumothorax results from medical procedures that breach the pleura, such as central venous catheter insertion, lung biopsy, or barotrauma from positive-pressure ventilation.
Effects on Lung Mechanics and Ventilation
As air accumulates within the pleural space, the affected lung recoils inward due to its natural elasticity. Lung volume on that side decreases, and alveoli collapse, reducing or abolishing ventilation to the affected region. The remaining lung tissue may initially compensate by increasing ventilation, but overall ventilatory efficiency declines as the proportion of non-functioning lung increases.
Loss of functional lung units reduces overall lung compliance, meaning greater effort is required to achieve adequate tidal volumes. Patients respond with tachypnoea and increased inspiratory effort, often accompanied by chest discomfort. In larger pneumothoraces, mediastinal structures may shift toward the opposite side, further impairing ventilation and increasing the work of breathing.
Ventilation–Perfusion Mismatch and Hypoxaemia
Pneumothorax creates areas of lung that are perfused but not ventilated. Blood continues to flow through capillaries adjacent to collapsed alveoli, producing regions of low ventilation relative to perfusion. This mismatch reduces arterial oxygen levels and contributes to hypoxaemia.
Hypoxic pulmonary vasoconstriction attempts to limit this effect by diverting blood away from non-ventilated regions toward better-ventilated lung. However, this response is often incomplete, particularly when collapse is extensive or develops rapidly. The degree of hypoxaemia therefore correlates with the size of the pneumothorax and the patient’s underlying pulmonary reserve.
Tension Pneumothorax and Haemodynamic Collapse
Tension pneumothorax represents the most severe form of pleural air accumulation. In this condition, air enters the pleural space during inspiration but cannot escape during expiration, creating a one-way valve effect. Intrapleural pressure rises progressively with each breath, compressing the affected lung and shifting the mediastinum toward the opposite side.
This mediastinal shift compresses the vena cavae and impairs venous return to the heart. As preload falls, cardiac output decreases, leading to hypotension and obstructive shock. Respiratory failure develops simultaneously due to severe lung compression and ventilation–perfusion mismatch. Without rapid decompression, cardiovascular collapse and cardiac arrest can occur.
Physiological Differences Between Simple and Tension Pneumothorax
In a simple pneumothorax, intrapleural pressure equilibrates with atmospheric pressure and remains relatively stable. Lung collapse is limited by this equilibrium, and haemodynamic compromise is uncommon, although gas exchange may still be impaired. In tension pneumothorax, intrapleural pressure continues to rise because trapped air cannot escape. The defining physiological difference is this progressive pressure accumulation, which drives both respiratory failure and circulatory collapse. Recognising this distinction is critical, as tension pneumothorax requires immediate decompression rather than observation or conservative management.
Clinical Connections
Pneumothorax typically presents with sudden onset dyspnoea and sharp, pleuritic chest pain resulting from irritation of the parietal pleura and acute loss of lung volume. Breath sounds are reduced or absent over the affected area, and percussion may reveal hyperresonance due to air within the pleural space. Oxygen saturation may be only mildly reduced in small pneumothoraces, particularly in people with healthy lungs, but hypoxaemia can be significant when collapse is extensive or when underlying lung disease limits compensatory capacity.
Several clinical features help estimate severity and urgency at the bedside:
Degree of respiratory distress and oxygen desaturation, reflecting loss of ventilated lung units
Unilateral chest findings, such as reduced expansion and absent breath sounds
Haemodynamic instability, which raises immediate concern for tension physiology
Chest imaging confirms the diagnosis by demonstrating air in the pleural space and partial or complete lung collapse. Plain chest radiography often shows a visible pleural line with absent lung markings beyond it, while CT may be used when the diagnosis is uncertain or complications are suspected. Management is guided by pneumothorax size, symptom burden, and physiological impact.
Small, stable pneumothoraces may be managed conservatively with observation and supplemental oxygen, while larger or symptomatic cases require intervention such as needle aspiration or intercostal drainage. Tension pneumothorax is a clinical diagnosis and demands immediate decompression, as delayed treatment risks rapid progression to respiratory failure and obstructive shock.
Concept Check
Why does air in the pleural space cause lung collapse?
How does pneumothorax impair ventilation–perfusion matching?
Why is hypoxaemia often worse in secondary pneumothorax?
How does tension pneumothorax lead to haemodynamic compromise?
What distinguishes a stable pneumothorax from a life-threatening one physiologically?