Pulmonary Surfactant
Pulmonary surfactant is one of the most vital substances in the respiratory system, yet its significance is often underestimated. Secreted by Type II alveolar cells, surfactant reduces surface tension within the alveoli, allowing them to remain open and stable throughout the respiratory cycle.
Without surfactant, breathing would require an enormous amount of effort, and gas exchange would be profoundly impaired. The discovery and study of surfactant transformed our understanding of respiratory physiology and revolutionised the care of premature infants and patients with acute lung injury. Its functions extend far beyond surface tension reduction, influencing lung mechanics, host defence, and the regulation of inflammation.
What You Need to Know
Surfactant is a complex mixture of phospholipids, neutral lipids, and specialised proteins. Its primary component, dipalmitoylphosphatidylcholine (DPPC), is exceptionally effective at lowering surface tension (the tendency of a liquid’s surface to resist stretching or spreading because the molecules are pulled more tightly toward each other) at the air–liquid interface. By reducing this tension, surfactant prevents alveoli from collapsing at the end of expiration, stabilising the lungs and reducing the work required to inflate them with each breath. This allows normal breathing to occur smoothly and efficiently.
If surfactant is destroyed or there is insufficient production:
acute respiratory distress syndrome (ARDS) can develop
alveolar collapse at end expiration (atelectasis)
work of breathing increases (more effort is required to open collapsed alveoli)
gas exchange decreases
pulmonary compliance reduces
Surfactant is stored within lamellar bodies inside Type II pneumocytes and is released into the alveolar space during breathing. Once secreted, it forms a thin molecular film that spreads across the alveolar surface. The presence of surfactant ensures that alveoli of different sizes remain open simultaneously; without it, smaller alveoli would collapse into larger ones because of differences in internal pressure, a phenomenon predicted by the Law of Laplace.
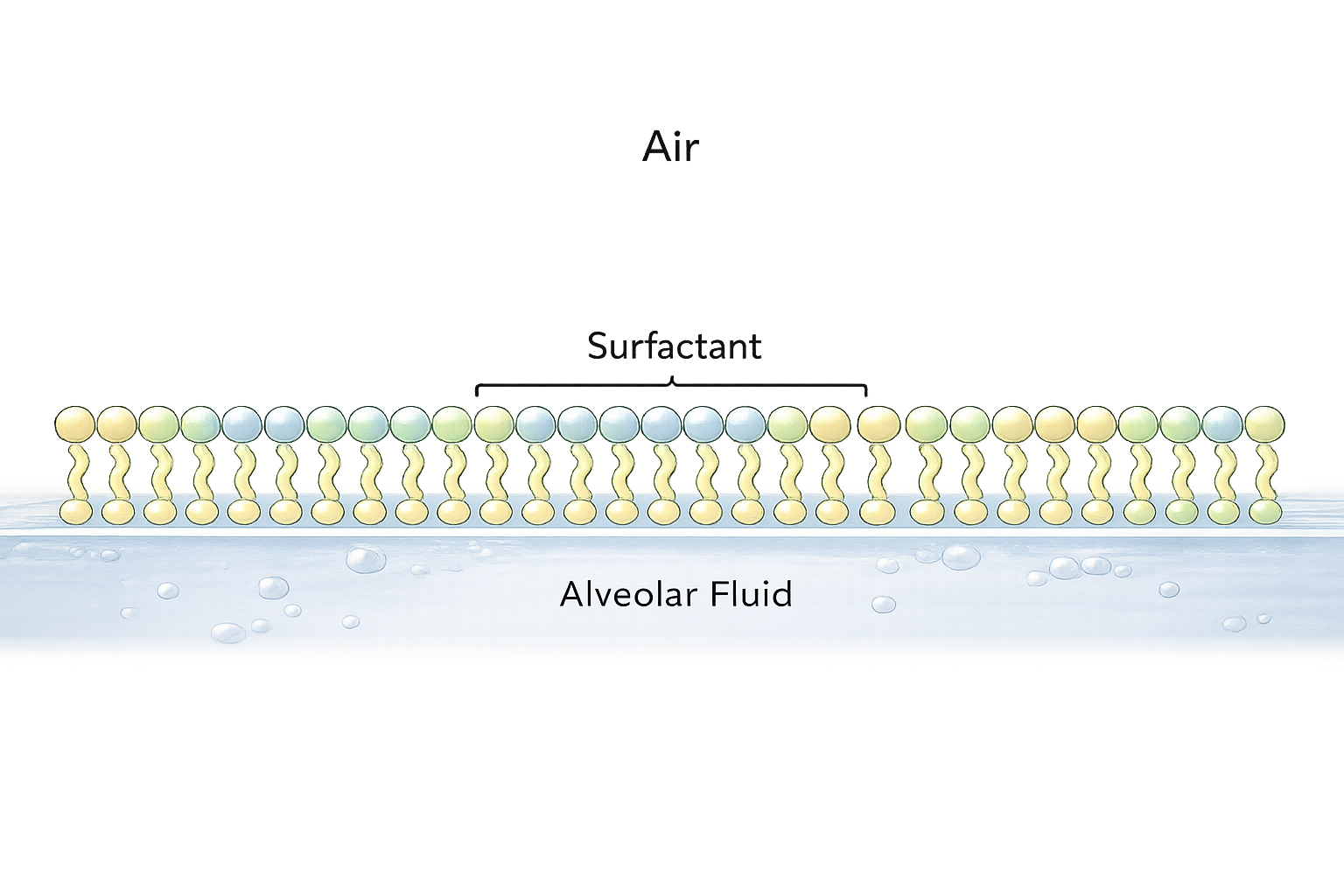
Image: Pulmonary surfactant forms a monolayer at the air–liquid interface, reducing surface tension and improving alveolar stability and lung compliance.
Beyond the Basics
Surfactant and Pulmonary Compliance
Pulmonary surfactant plays a critical role in determining lung compliance. By reducing surface tension at the air–liquid interface within the alveoli, surfactant prevents alveolar collapse and allows the lungs to expand more easily during inspiration. This reduction in surface tension lowers the pressure required to inflate the alveoli, decreasing the work of breathing and improving ventilatory efficiency.
When surfactant is absent or dysfunctional, lung compliance falls dramatically. The alveoli become stiff and unstable, requiring significantly greater inspiratory effort to achieve adequate ventilation. This is seen in conditions such as neonatal respiratory distress syndrome (NRDS), where surfactant deficiency is primary, and in acute respiratory distress syndrome (ARDS), where surfactant is inactivated or depleted due to acute lung injury. In these states, patients often adopt rapid, shallow breathing patterns in an attempt to minimise the energy cost of ventilation, increasing the risk of respiratory muscle fatigue and failure.
Immunological Functions of Surfactant
In addition to its mechanical effects, surfactant plays an essential role in pulmonary host defence. Specific surfactant-associated proteins contribute to innate immunity within the alveolar environment.
Surfactant proteins A and D:
Bind to bacteria, viruses, and fungi
Enhance recognition and phagocytosis by alveolar macrophages
Modulate inflammatory signalling to limit excessive tissue injury
Through these mechanisms, surfactant acts as a first-line defence, helping neutralise inhaled pathogens before infection becomes established. This dual mechanical and immunological function highlights the importance of surfactant in preserving alveolar integrity.
Surfactant Production, Recycling, and Injury
Surfactant homeostasis is tightly regulated by alveolar type II epithelial cells. These cells synthesise surfactant components, secrete them onto the alveolar surface, and continuously recycle surfactant through reuptake and reuse. This dynamic process ensures that the surfactant layer remains functional despite the constant mechanical stress of breathing.
During lung injury, this cycle becomes disrupted. Inflammatory processes increase capillary permeability, allowing protein-rich fluid to enter the alveoli. These proteins interfere with surfactant’s ability to reduce surface tension, while simultaneous damage to type II cells reduces surfactant synthesis. The combination of inactivation and reduced production leads to alveolar instability, collapse, and impaired gas exchange.
This disruption is a central feature of ARDS, where widespread surfactant dysfunction contributes to refractory hypoxaemia and decreased lung compliance.
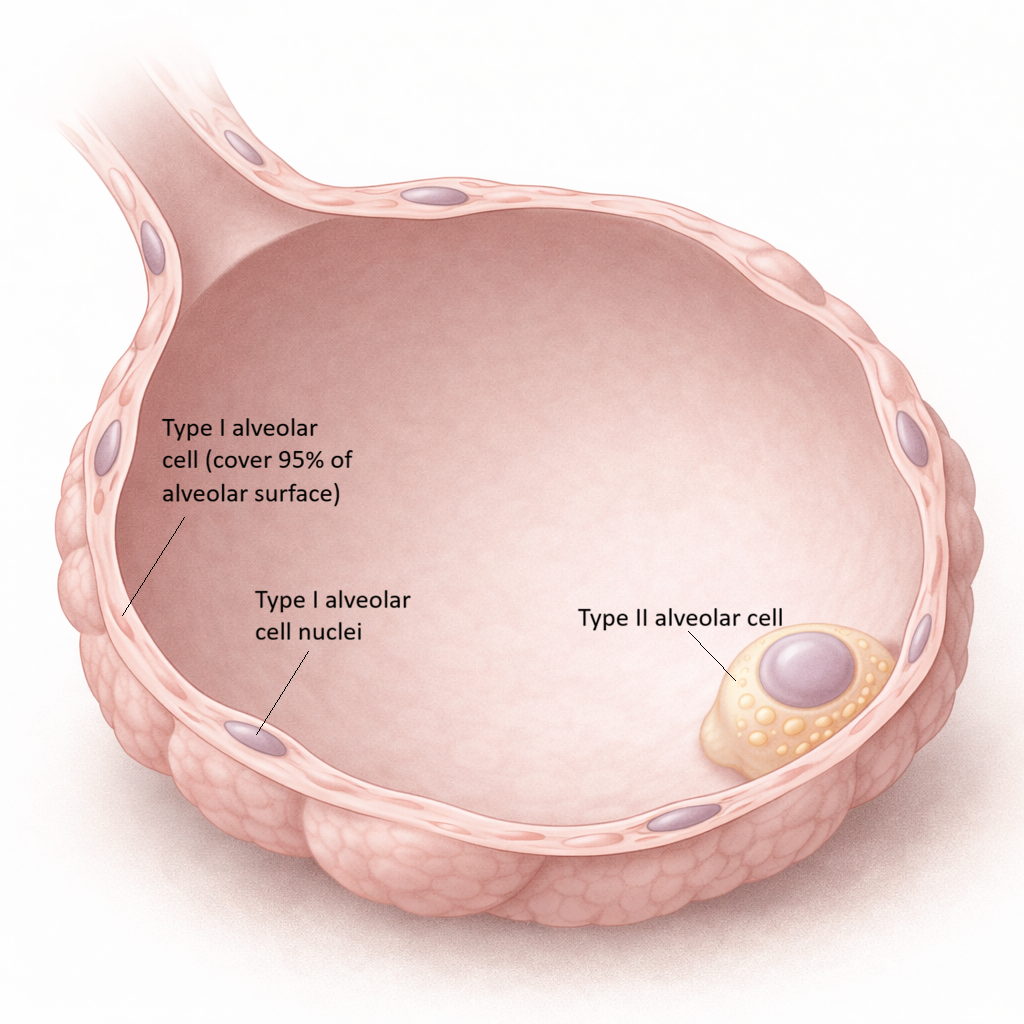
Image: Alveolar structure. The alveolar wall is formed by thin Type I cells that facilitate gas exchange, while scattered Type II cells produce surfactant to maintain alveolar stability.
Mechanical Ventilation and Surfactant Function
Mechanical ventilation (when a ventilator is used to assist or take over breathing) can significantly influence surfactant integrity. High tidal volumes and repetitive alveolar overdistension can damage type II cells and disrupt surfactant distribution, exacerbating lung injury. Conversely, appropriate ventilatory strategies can help preserve surfactant function.
Positive end-expiratory pressure (PEEP) plays a key role by preventing alveolar collapse at end-expiration. By maintaining alveolar patency, it supports even distribution of surfactant across the alveolar surface, improves compliance, and reduces cyclic opening and closing of alveoli. This protective effect underpins lung-protective ventilation strategies used in conditions such as ARDS.
Clinical Connections
Surfactant deficiency is most classically seen in premature infants, where Type II alveolar cells are not yet fully mature. Without adequate surfactant, alveoli collapse with each exhalation, making breathing extremely difficult and energetically costly. The introduction of exogenous surfactant therapy, delivered directly into the lungs, has dramatically improved outcomes in neonatal respiratory distress syndrome by restoring alveolar stability and improving lung compliance.
Key clinical patterns include:
Prematurity → inadequate surfactant production → alveolar collapse
ARDS → impaired surfactant function due to inflammation and fluid
Chronic lung disease → altered surfactant distribution or composition
Shallow breathing → reduced surfactant spread → increased atelectasis risk
In adults, surfactant dysfunction is a hallmark of acute respiratory distress syndrome (ARDS). Inflammation, alveolar injury, and fluid accumulation disrupt both the production and function of surfactant, leading to stiff, non-compliant lungs that are difficult to ventilate. This underpins the use of positive end-expiratory pressure (PEEP), which helps maintain alveolar recruitment and counteracts the effects of surfactant loss.
Chronic lung conditions can also impair surfactant dynamics. In pulmonary fibrosis, distortion of alveolar architecture interferes with even surfactant distribution. In smokers, exposure to toxins alters surfactant composition and contributes to macrophage dysfunction, reducing both mechanical stability and host defence.
Surfactant physiology also explains the importance of deep breaths. Periodic sighs or intentional deep inspirations help redistribute surfactant across the alveolar surface. In contrast, prolonged shallow breathing, such as during pain, sedation, or immobility, promotes alveolar collapse and reduces surfactant effectiveness, increasing the risk of atelecta
Concept Check
How does surfactant stabilise alveoli of different sizes?
Why does surfactant deficiency lead to stiff, non-compliant lungs?
How do surfactant proteins contribute to innate immunity?
Why is surfactant dysfunction a major contributor to ARDS?
What role does PEEP play in supporting surfactant function?