Respiratory Muscle Physiology
Breathing depends not only on the lungs but also on the coordinated activity of several muscle groups that generate the pressure changes required for ventilation. These muscles perform an extraordinary task: they must function continuously throughout life, remain adaptable to changes in activity or metabolic demand, and respond rapidly during stress, illness, or exertion.
Understanding the physiology of the respiratory muscles provides a deeper appreciation of how ventilation is maintained, why respiratory fatigue occurs, and how certain conditions compromise the mechanics of breathing. It also explains why patients in respiratory distress adopt characteristic postures, rely heavily on accessory muscles, or reach the point where breathing becomes unsustainable without support.
What You Need to Know
The diaphragm is the primary muscle of inspiration and accounts for the majority of ventilation at rest. When it contracts, it flattens and moves downward, increasing the vertical dimension of the thoracic cavity and lowering intrathoracic pressure. This pressure gradient draws air into the lungs in a smooth and efficient manner. The diaphragm is highly fatigue-resistant due to its rich blood supply and high proportion of oxidative muscle fibres, an adaptation essential for its continuous activity.
The key muscle actions include:
Quiet inspiration: diaphragm contracts and descends to increase vertical thoracic volume; external intercostals elevate the ribs, expanding the thoracic cavity laterally and anteriorly
Forced inspiration: sternocleidomastoid elevates the sternum; scalenes elevate the upper ribs; pectoralis minor assists in lifting the ribcage when the upper limb is fixed, further increasing thoracic volume
Passive expiration: diaphragm relaxes and recoils upward while the lungs and chest wall elastically recoil, reducing thoracic volume without active muscle contraction
Forced expiration: abdominal muscles contract to increase intra-abdominal pressure, pushing the diaphragm upward; internal intercostals depress the ribs to actively decrease thoracic volume and accelerate airflow out of the lungs
Assisting the diaphragm are the external intercostal muscles, which elevate the ribs and expand the thoracic cavity laterally and anteriorly. This coordinated movement increases intrathoracic volume and complements diaphragmatic action during quiet breathing. During deeper or more demanding breaths, accessory muscles, including the sternocleidomastoid, scalene muscles, and pectoralis minor, become active, lifting the sternum and upper ribs to augment ventilation. Their involvement is minimal in healthy individuals at rest but becomes prominent in exercise or respiratory distress.
Expiration during quiet breathing is passive, relying on the elastic recoil of the lungs and chest wall. However, during forced breathing or when resistance is increased, such as in asthma or COPD, abdominal muscles and internal intercostals contract to actively decrease thoracic volume and accelerate air movement out of the lungs.
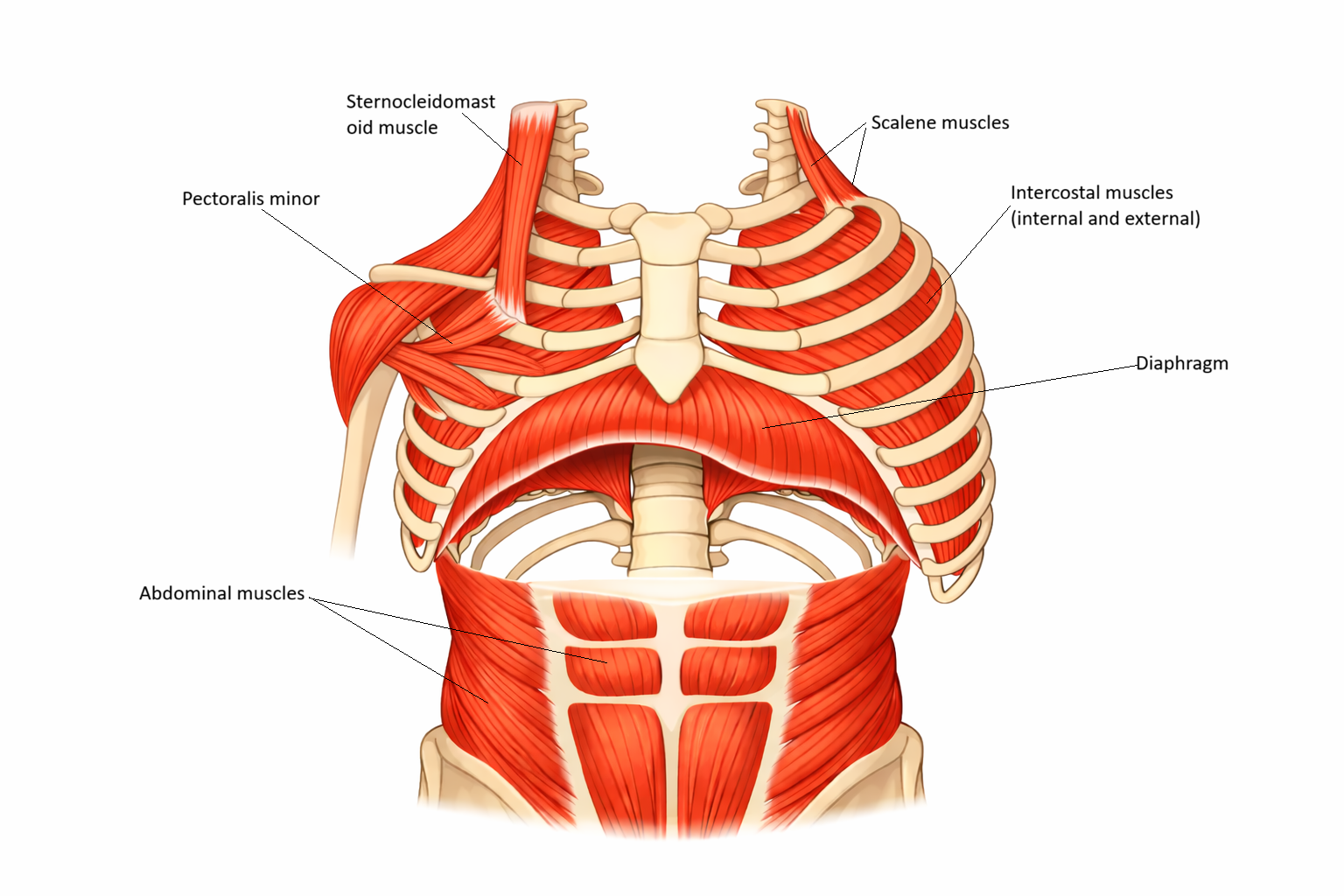
Image: Primary and accessory muscles of respiration. The diaphragm forms the base of the thoracic cavity, while intercostals stabilise and move the ribs. Accessory muscles, including the sternocleidomastoid and pectoralis minor, assist during increased respiratory demand by elevating the ribcage.
Beyond the Basics
Functional Demands of the Respiratory Muscles
The respiratory muscles must operate continuously, balancing strength, endurance, and mechanical efficiency to sustain ventilation under a wide range of physiological conditions. Unlike limb muscles, which can rest between contractions, respiratory muscles must remain active at all times. Their structure and fibre composition reflect the need for sustained, low-energy activity rather than short bursts of maximal force.
Under resting conditions, the energetic cost of breathing is relatively low. However, as respiratory load increases, the demand placed on these muscles rises rapidly, making efficiency a critical determinant of ventilatory success.
The Diaphragm: Mechanics and Length–Tension Relationship
The diaphragm is the primary muscle of inspiration. Its dome-shaped structure allows it to generate large changes in intrathoracic pressure with relatively small movements, minimising the energy cost of breathing. As the diaphragm contracts, it descends and flattens, increasing thoracic volume and drawing air into the lungs.
Diaphragmatic efficiency depends on the length–tension relationship. At optimal resting lung volumes, diaphragm muscle fibres are positioned to generate maximal force. As lung volume increases, the diaphragm flattens and shortens, reducing its ability to develop tension. This mechanical disadvantage explains the marked breathlessness experienced by patients with chronic hyperinflation, such as those with emphysema. In these individuals, the diaphragm operates at a persistently shortened length, limiting inspiratory force generation and increasing the work of breathing.
Accessory Muscle Recruitment and Increased Work of Breathing
When diaphragmatic efficiency is reduced or ventilatory demand increases, accessory muscles are recruited to assist inspiration. These include the sternocleidomastoid, scalene, and upper chest wall muscles. While accessory muscle use can temporarily support ventilation, it is far less efficient than diaphragmatic breathing and substantially increases energy expenditure.
Persistent recruitment of accessory muscles at rest reflects an elevated work of breathing and reduced respiratory reserve. Over time, this compensatory strategy contributes to respiratory muscle fatigue and ventilatory failure.
Intercostal Muscles and Chest Wall Stability
The intercostal muscles contribute to ventilation by elevating the ribs during inspiration and stabilising the chest wall during pressure changes. Their stabilising function is essential; without adequate intercostal tone, the negative pressure generated during inspiration would cause inward collapse of the chest wall rather than effective lung expansion.
Dysfunction of the intercostal muscles, such as from spinal cord injury, thoracic trauma, or neuromuscular disease, reduces chest wall rigidity. This impairs tidal volume generation and shifts a greater burden onto the diaphragm and accessory muscles, further increasing the work of breathing.
Abdominal Muscles and Expiratory Function
Abdominal muscles play a vital role during forced expiration, coughing, and airway clearance. Contraction of these muscles increases intra-abdominal pressure, pushing the diaphragm upward and generating the high expiratory airflow required to mobilise and expel secretions.
When abdominal muscle strength is reduced — due to neuromuscular disease, spinal cord injury, or prolonged mechanical ventilation — cough effectiveness declines. This predisposes patients to secretion retention, atelectasis, and pneumonia, particularly during acute illness.
Neural Control of Respiratory Muscle Function
Effective respiratory muscle activity depends on intact neural control. The diaphragm is innervated by the phrenic nerves, while intercostal and accessory muscles rely on thoracic spinal nerves. Coordination between central respiratory centres and peripheral motor pathways ensures synchrony between muscle contraction and lung inflation.
Neurological injury, impaired central drive, or neuromuscular disease can therefore compromise ventilation even when muscle structure itself is intact. This highlights the close integration between respiratory mechanics and neural regulation.
Respiratory Muscle Fatigue and Oxygen Cost of Breathing
Although the diaphragm is highly fatigue-resistant, respiratory muscles are vulnerable to fatigue during sustained increases in workload. Conditions such as severe asthma, pneumonia, sepsis, or ARDS markedly increase the effort required for ventilation. As respiratory muscle work rises, so too does their oxygen consumption.
Under these conditions, a growing proportion of total oxygen delivery is diverted to the respiratory muscles themselves, reducing availability for other vital organs. As fatigue develops, breathing becomes rapid and shallow, tidal volume falls, and carbon dioxide retention may ensue. If this process is not recognised early, progressive respiratory muscle failure and ventilatory collapse can occur.
Clinical Connections
Many clinical conditions disrupt respiratory muscle function. In COPD, chronic hyperinflation alters the diaphragm’s shape, reducing its strength and placing a greater burden on accessory muscles. These patients often use pursed-lip breathing and forward-leaning postures to improve mechanical efficiency and delay airway collapse. In neuromuscular disorders such as muscular dystrophy, Guillain–Barré syndrome, or motor neurone disease, progressive muscle weakness impairs ventilation, reduces cough strength, and ultimately leads to respiratory insufficiency.
Spinal cord injuries above the level of the phrenic nerve (C3–C5) paralyse the diaphragm entirely, necessitating ventilatory support. Injuries below this level may spare diaphragmatic function but impair intercostal and abdominal muscle activity, reducing cough effectiveness and leading to secretion retention. Opioid overdose represents another major cause of respiratory muscle suppression, as these drugs depress the neural drive to breathe.
In critically ill patients, prolonged mechanical ventilation can cause diaphragmatic atrophy due to disuse, a phenomenon known as ventilator-induced diaphragmatic dysfunction. This weakness complicates weaning and prolongs the need for respiratory support. Early rehabilitation strategies and careful ventilator settings can help mitigate this risk.
Concept Check
Why does the diaphragm become less effective in patients with lung hyperinflation?
How do accessory muscles assist ventilation during respiratory distress?
Why are abdominal muscles essential for an effective cough?
How does neuromuscular disease impair respiratory function even when lung tissue is normal?
What factors contribute to respiratory muscle fatigue in acute illness?