Recognising Patient Deterioration
Nurses play a critical role in recognising patient deterioration. While severe deterioration may appear sudden, it is often preceded by physiological changes that can be detected with thorough assessment and clinical awareness. Signs of deterioration are often evident anywhere from hours to days prior to a cardiac arrest. Common signs of deterioration include, but are not limited to, tachycardia, hypotension, tachypnoea, reduced oxygen saturation, and an altered conscious state. Recognising signs of deterioration early has been proven to improve outcomes, prevent cardiopulmonary arrest, and reduce hospital mortality rates.
What You Need to Know
Recognising patient deterioration is about identifying early physiological changes before they progress to organ failure and cardiac arrest. Although sudden cardiac arrest (SCA) with no prior warning signs can occur, this is rare. Deterioration is rarely sudden and without warning. Subtle trends in observations, behaviour, and clinical appearance often occur hours before a critical event. The nurse’s role is to notice these changes, use clinical judgment, and escalate care appropriately.
Track and Trigger
Track and trigger systems are used in many healthcare settings globally to support early recognition of patient deterioration. Observations such as heart rate, blood pressure, respiratory rate, oxygen saturation, temperature, and level of consciousness are recorded and tracked over time. Each vital sign recorded on the observation chart sits within a ‘zone’ which either signifies no action is required, or triggers a specific clinical response, such as a rapid medical review or a more urgent Medical Emergency Team (MET) review. Many observation charts now also use a scoring system, where recorded vital signs are mapped to a scoring system, with the final score indicating if escalation of care is warranted.
These systems rely on both single abnormal values and trends. A patient may trigger a response from one significantly abnormal observation or from multiple smaller changes across different parameters. For example, if a patient’s blood pressure suddenly decreased to 80/45mmHg, it would not be appropriate to wait to identify a trend in vital signs, a single abnormal value can warrant immediate escalation. This system was introduced to improve early detection of patient deterioration and reduce reliance on subjective clinical judgement by providing clear, standardised triggers for escalation.
Paper-based and Electronic Observation Charts
Observation charts are typically colour coded to make this process clear and actionable. Each chart details instructions on what response should occur, depending on which coloured zone the vital sign has been recorded in. Yellow zones indicate that the patient requires increased monitoring, orange zones indicate an urgent clinical review is required, usually by a medical officer or senior clinician, and red zones indicate that the patient meets criteria for a MET call. Electronic medical records (EMR) identify deterioration by automatically analysing entered observations, flagging abnormal values, trends, and trigger thresholds to prompt clinical review or escalation.
Medical Emergency Team (MET)
A MET call initiates urgent escalation for patients with acute or life threatening deterioration. It brings a critically care trained ICU team (an ICU nurse and senior ICU doctor), to the bedside to provide immediate assessment and intervention. This allows advanced life support to be delivered early, before cardiac arrest or further deterioration occurs. In the event that a MET call progresses to cardiac arrest, the ICU MET team are trained to deliver advanced resuscitation care.
Patients may have altered MET criteria based on their baseline condition or clinical context. For example, if a patient is known to have borderline, asymptomatic hypotension as their baseline, the treating medical team may document that a MET call is only required if their vital signs are within certain parameters (parameters to be clearly communicated and documented by the treating senior doctor). Altered MET call criteria must be clearly documented by a senior doctor and should not delay escalation if the patient is clinically deteriorating.
While track and trigger systems provide clear guidance, they do not replace clinical judgement. A patient who appears unwell or is showing concerning trends should be escalated even if formal criteria have not yet been met.
Early signs that should raise concern include:
Increasing heart rate, even within normal limits, as a compensatory response to maintain cardiac output
Subtle drops in blood pressure or narrowing pulse pressure
Rising respiratory rate, often the earliest and most sensitive indicator
Changes in mental state such as restlessness, confusion, or reduced alertness
Reduced urine output, indicating declining renal perfusion
Skin changes such as pallor, cool peripheries, or delayed capillary refill
These changes often occur before obvious instability. Recognising them early allows intervention before decompensation occurs.
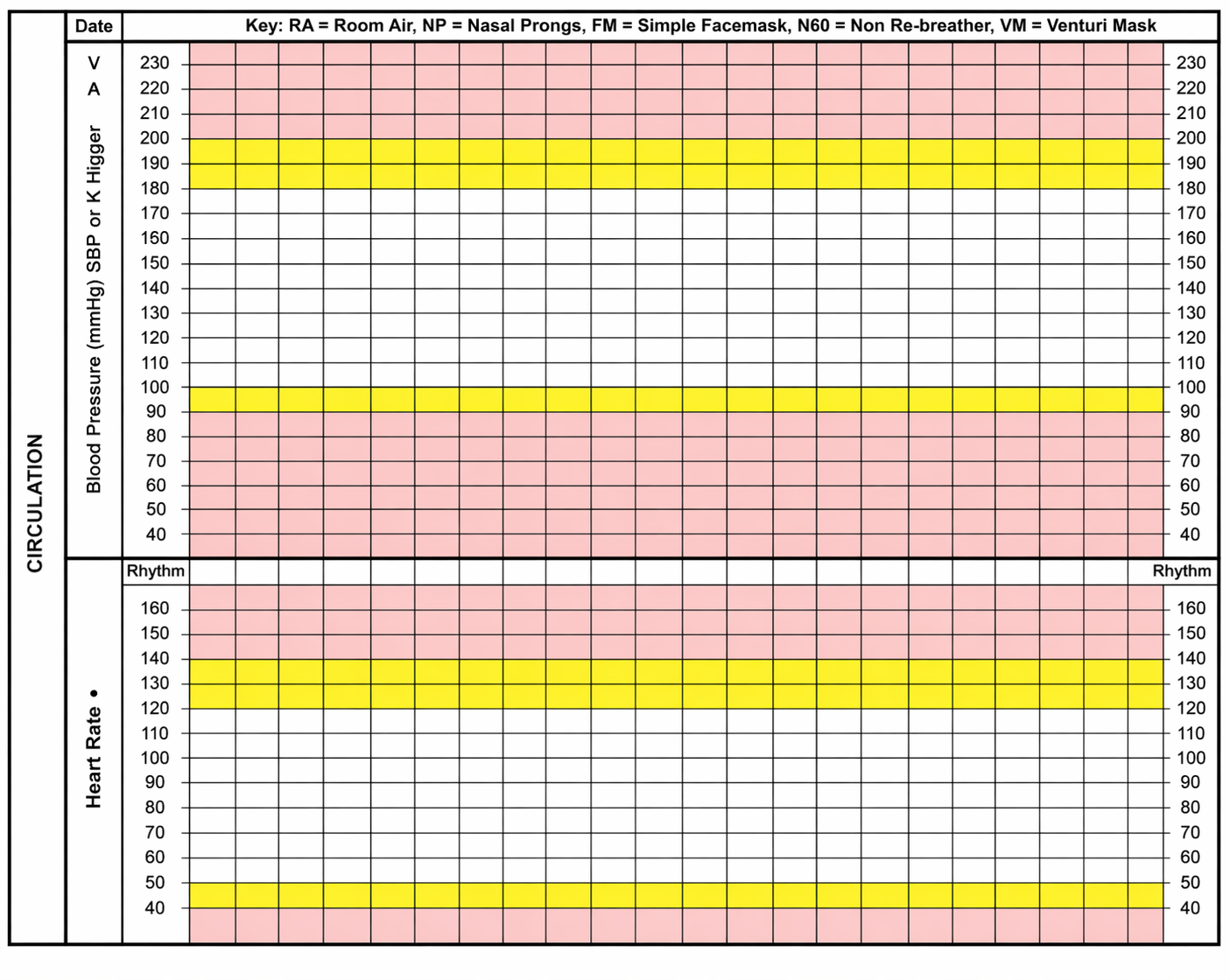
Image: An example of a colour coded observation chart to support early recognition of deterioration. While formats vary between organisations, yellow zones generally indicate the need for urgent clinical review or increased monitoring, and red zones correspond to MET call criteria.
Beyond the basics
Physiological compensation can mask deterioration until the patient reaches a critical point. The body initially maintains perfusion through mechanisms such as tachycardia, vasoconstriction, and increased respiratory effort. These responses can keep observations within a “normal” range despite worsening pathology, which is why early deterioration is often missed.
Blood pressure and MAP
A falling systolic blood pressure or mean arterial pressure (MAP) indicates reduced organ perfusion. MAP is the key driver of blood flow to vital organs. Once it falls to around 65 mmHg, autoregulation (an organ’s ability to maintain relatively constant blood flow, despite variations in systemic pressure) begins to fail, and organs such as the brain, heart, and kidneys can no longer maintain consistent blood flow. Below this point, perfusion becomes pressure dependent, so even small drops can result in a rapid decline in oxygen delivery. This is why a patient can appear stable and then deteriorate quickly once this threshold is crossed.
Heart rate
Heart rate is often one of the earliest compensatory changes. An increasing heart rate helps maintain cardiac output when stroke volume falls, such as in hypovolaemia or early shock. A rising trend, even within normal limits, can be clinically significant. A sudden drop in heart rate in an unwell patient is particularly concerning, as it may indicate failure of compensatory mechanisms or impending collapse.
Respiratory rate and work of breathing
Respiratory rate is the most sensitive early indicator of deterioration because it responds quickly to physiological stress. Despite its importance, respiratory rate is frequently estimated rather than counted, making it the most commonly fabricated observation. This can delay recognition of early deterioration. It often rises before changes in oxygen saturation or blood pressure as the body compensates for hypoxia, metabolic acidosis, or poor perfusion. However, assessment must go beyond rate alone.
The rhythm and pattern of breathing provide important clinical information. Irregular breathing, periods of apnoea, or laboured breathing suggest worsening respiratory or neurological compromise. Increased work of breathing, such as use of accessory muscles, nasal flaring, or inability to speak in full sentences, indicates that the patient is struggling to maintain adequate ventilation.
Abnormal breath sounds are also significant and should be reported immediately. Stridor suggests upper airway obstruction and is a medical emergency. Wheeze may indicate lower airway narrowing, while crackles can suggest fluid in the alveoli. These findings help identify the cause of deterioration and guide urgency of intervention.
Oxygen saturation
Oxygen saturation should not be used in isolation to assess respiratory status. A patient may maintain normal saturations while deteriorating, particularly if they are receiving supplemental oxygen. A falling saturation, increasing oxygen requirements, or inability to maintain target saturations all require urgent escalation.
Temperature
Temperature can indicate infection, inflammation, or impaired thermoregulation. Fever may be an early sign of sepsis, but a low temperature can be equally concerning, particularly in older adults, immunocompromised patients, or those with severe infection. Hypothermia is significant because reduced body temperature slows cellular metabolism and enzyme activity, impairing oxygen delivery, coagulation, and organ function.A patient who is hypothermic, clammy, or peripherally cool despite being unwell may have poor perfusion and reduced physiological reserve.
Mental state
Changes in mental state are an early indicator of cerebral hypoperfusion or hypoxia. The brain is highly sensitive to reduced oxygen delivery, so agitation, confusion, or decreased responsiveness may occur early. Any new or worsening change should be treated as significant and prompt further assessment.
Recognising deterioration requires looking at the full pattern. Trends across multiple observations, even if individually subtle, often indicate a patient who is becoming unstable. A single observation may not appear critical on it’s own when within normal parameters, but a consistent change over time is clinically significant. For example, a gradual rise in heart rate combined with a slow fall in blood pressure and increasing respiratory rate indicates a deteriorating trajectory, even if each value individually appears acceptable.
In practice
In clinical settings, recognising deterioration requires active observation, pattern recognition, and timely escalation. This involves not only recording vital signs but interpreting what they mean in context. Signs of deterioration can be missed because early changes can be subtle, but also due to inexperience or lack of confidence in recognising and interpreting abnormal findings. This is why it is essential for nurses to learn how to recognise and interpret early signs of deterioration, so they can act promptly and prevent further clinical decline.
When assessing a patient, interpret observations alongside clinical presentation. Patients often show objective signs of deterioration before values become markedly abnormal, such as increased work of breathing, altered mental state, or changes in perfusion. These physiological cues should prompt further assessment and escalation, even if observations are still within normal limits.
Key actions in practice include:
Comparing current observations to baseline data
Identifying early compensatory changes such as tachycardia or increased respiratory effort
Recognising when values are approaching critical thresholds, particularly MAP around 65 mmHg
Assessing for associated signs, such as reduced urine output or altered mental state
Acting early rather than waiting for severe abnormalities
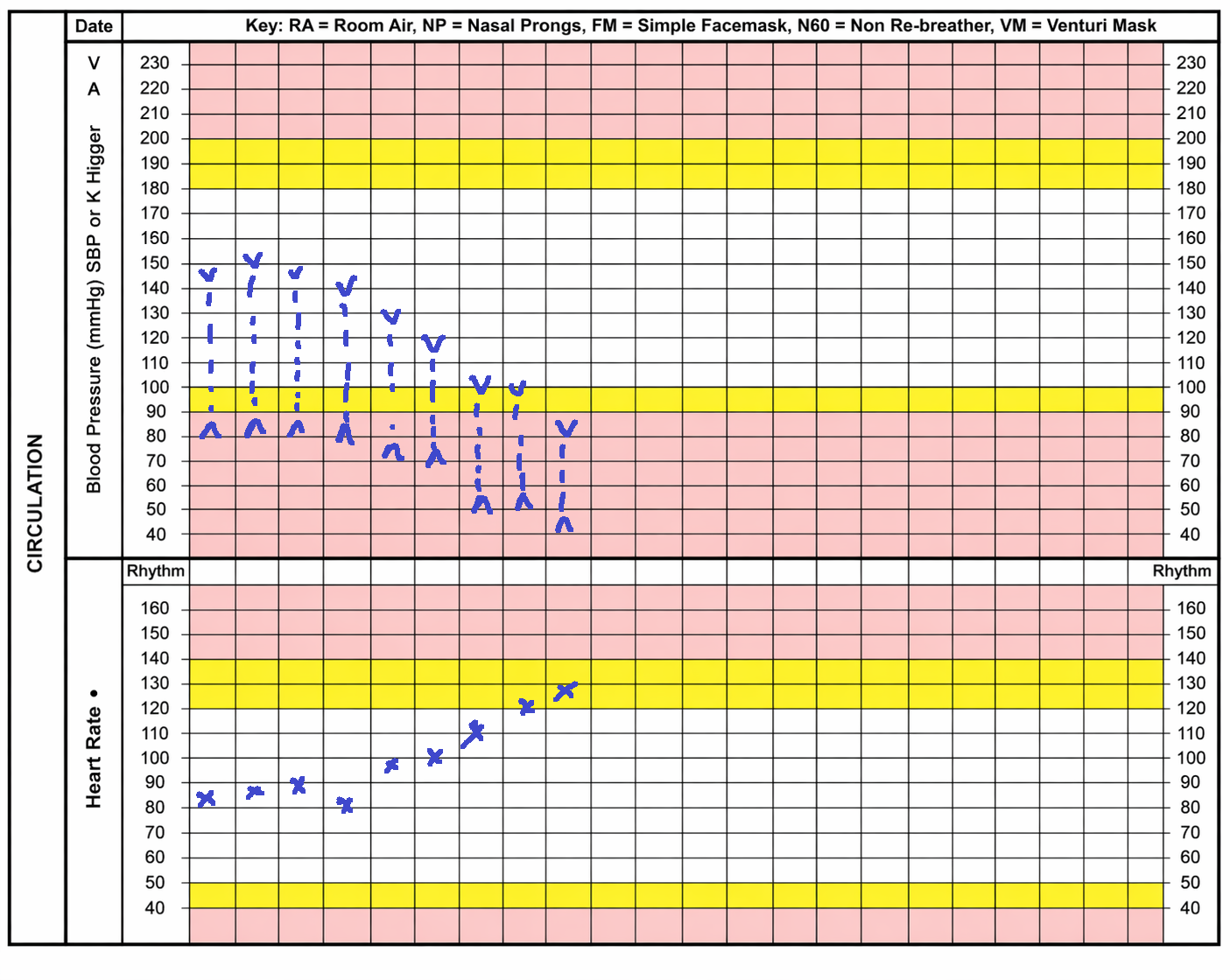
Image: Note the down trending blood pressure and up trending heart rate. The final recording of the blood pressure is within the MET zone and the final recording of the heart rate is within the rapid review zone. While not all deterioration will be this obvious, this is an example of a trend progressing to MET criteria.
Escalation and Documentation
Nurses new to a clinical environment should familiarise themselves with local escalation processes, including how to activate a MET call or code blue, where emergency call systems are located, and who to escalate to if they are concerned but unsure whether formal criteria are met.
Documentation is also critical. Observations should be recorded accurately and accompanied by clear descriptions of clinical changes. Examples of documentation that provides a vague depiction of patient status are:
provides no clinical detail (e.g. “appears unwell”)
does not include what action was taken (i.e. who did the nurse escalate to, what was the response, what intervention was recommended, what was implemented, and was it effective?)
does not include an accurate time for deteriorations events, including escalation (e.g. was there progression of deterioration? What time was deterioration noted? What time was it escalated? What time were interventions implemented? What time was improvement noted?)
Documentation should specify what has changed, when it changed, and what actions were taken. Documenting all aspects of deterioration ensures trends are clearly communicated, escalation decisions are supported with objective evidence, and there is an accurate record of what was identified, when, and how it was managed.