CARDIAC TAMPONADE: Acute Compression of the Heart Leading to Impaired Ventricular Filling
Cardiac tamponade is a life-threatening condition that occurs when fluid accumulation within the pericardial sac increases intrapericardial pressure to the point that it restricts cardiac filling. As the heart becomes compressed, diastolic filling is impaired, stroke volume falls and cardiac output rapidly declines. Unlike chronic pericardial effusions, which may be well tolerated for long periods, tamponade is defined by the rate of fluid accumulation rather than absolute volume. Cardiac tamponade leads to severe haemodynamic compromise and requires immediate recognition and intervention. Without prompt treatment, the condition progresses to obstructive shock and death.
What You Need to Know
Cardiac tamponade occurs when fluid builds up within the pericardial sac and begins to compress the heart. The pericardium is normally a thin, flexible layer with a small amount of fluid that allows the heart to move smoothly. When excess fluid accumulates, pressure within this space rises and restricts the heart’s ability to expand during diastole, which is when the ventricles fill with blood.
As filling becomes impaired, less blood enters the ventricles, leading to a reduction in stroke volume and cardiac output. This means that even though the heart may be beating faster in response, it is pumping less effectively with each contraction. The body attempts to compensate through tachycardia and vasoconstriction, but these responses cannot overcome the mechanical compression of the heart.
The key features of cardiac tamponade can be summarised as follows:
External pressure on the heart limits ventricular filling
Reduced preload leads to decreased stroke volume and cardiac output
Compensatory tachycardia and vasoconstriction attempt to maintain perfusion
Progression can lead to obstructive shock if untreated
The severity of tamponade depends largely on how quickly fluid accumulates. Slow accumulation may allow the pericardium to stretch and accommodate larger volumes with fewer immediate effects. In contrast, rapid fluid accumulation causes a sudden rise in pressure, meaning even small volumes can significantly impair cardiac function. Without prompt recognition and intervention, cardiac tamponade can rapidly progress to haemodynamic instability and cardiovascular collapse.
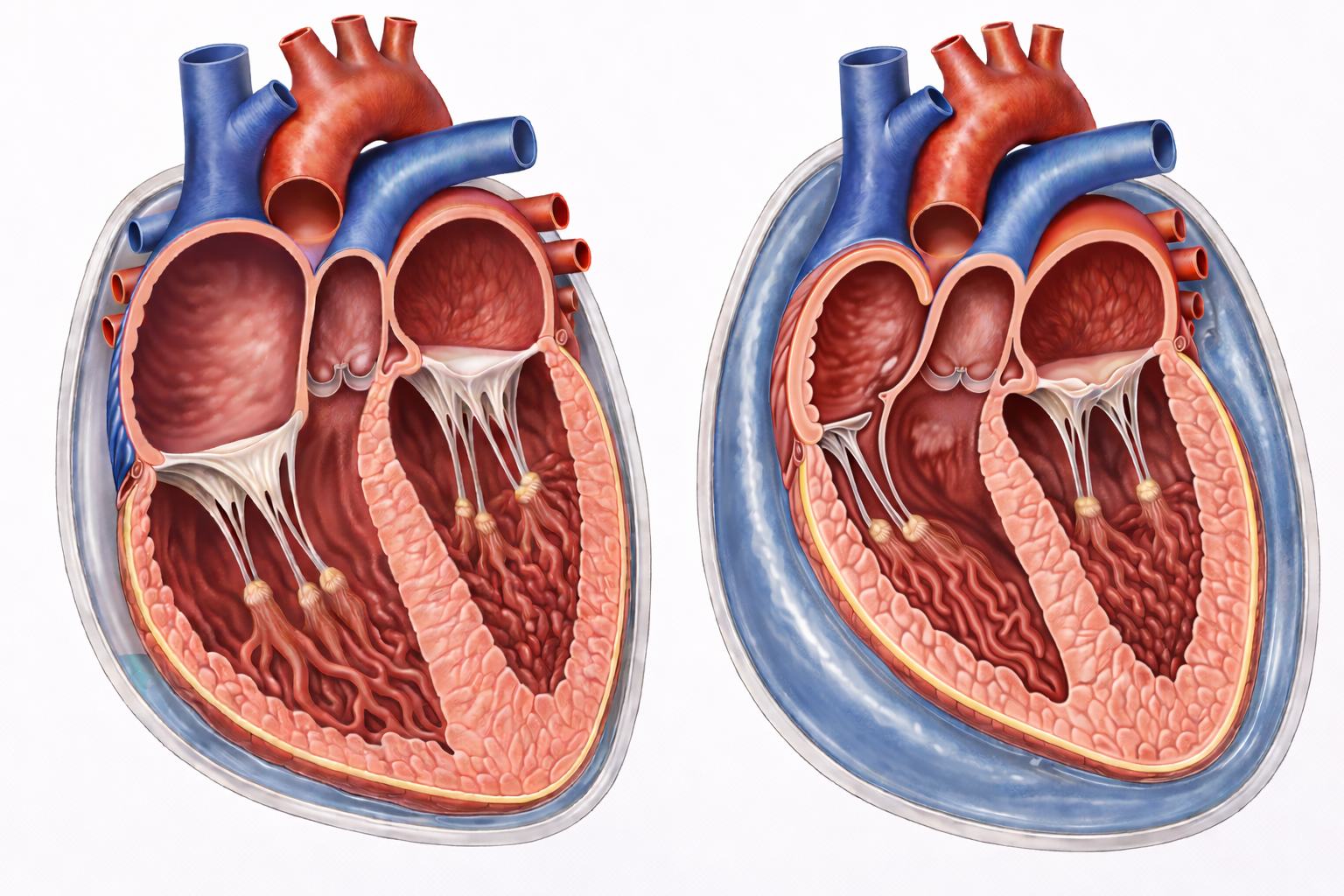
Image: Left: normal heart with minimal pericardial fluid.
Right: increased pericardial fluid compresses the right atrium and right ventricle, limiting cardiac filling.
Beyond the Basics
Pathophysiological mechanism of tamponade
Cardiac tamponade occurs when fluid within the pericardial sac raises intrapericardial pressure (pressure inside the pericardial space) to the point that it restricts normal cardiac filling. As this pressure rises, it begins to exceed the low pressures within the right atrium and right ventricle during diastole (the relaxation phase when the heart fills with blood). This prevents the chambers from expanding properly.
Because the ventricles cannot fill, preload (the volume of blood entering the heart before contraction) falls, leading to reduced stroke volume and cardiac output. Although the body attempts to compensate by increasing heart rate and constricting blood vessels, these responses cannot overcome the external compression. For this reason, tamponade is classified as a form of obstructive shock, where blood flow is limited by a physical barrier rather than a loss of volume.
Rate of fluid accumulation
The severity of tamponade depends more on how quickly fluid accumulates than on the total volume present. When fluid collects slowly, the pericardium (a relatively stiff but slightly stretchable sac) can gradually adapt, allowing larger volumes to accumulate before pressure rises significantly.
In contrast, rapid accumulation causes a sharp rise in pressure because the pericardium has no time to stretch. Even small volumes can then severely impair cardiac filling. This explains why acute causes, such as trauma or myocardial rupture, can lead to sudden haemodynamic collapse, while chronic effusions may remain stable until a critical threshold is reached.
Ventricular interdependence and pulsus paradoxus
Within the confined pericardial space, the ventricles compete for limited room to fill, a concept known as ventricular interdependence. During inspiration, increased venous return to the right ventricle causes it to expand. In tamponade, this expansion cannot occur outward, so the interventricular septum shifts toward the left ventricle instead.
This shift reduces left ventricular filling and lowers stroke volume during inspiration. The clinical manifestation of this is pulsus paradoxus, an exaggerated drop in systolic blood pressure during inspiration. While a small decrease is normal, in tamponade the reduction is more pronounced due to the restricted filling of the left ventricle.
Pressure–volume relationship
The pericardium has limited elasticity, and its response to fluid accumulation follows a pressure–volume relationship. Initially, small increases in fluid cause minimal rises in pressure as the pericardium stretches. However, once this reserve capacity is exceeded, the curve becomes steep, meaning that even small additional volumes lead to large increases in pressure.
This explains why patients can remain stable for a period and then deteriorate rapidly once a critical point is reached. The key factor is not the absolute volume of fluid, but how much the pericardium can accommodate before pressure rises sharply.
Chamber collapse and haemodynamic consequences
As intrapericardial pressure increases, it preferentially compresses the right-sided chambers first because they operate at lower pressures. This leads to diastolic collapse of the right atrium and right ventricle, meaning these chambers are unable to remain open during filling.
The result is impaired venous return, elevated jugular venous pressure, and reduced cardiac output. As stroke volume falls, hypotension develops, and the body compensates with tachycardia and vasoconstriction. However, without relieving the pressure, these mechanisms are insufficient, and organ perfusion becomes compromised.
Progression to shock and collapse
If tamponade is not relieved, ongoing restriction of ventricular filling leads to progressive reduction in cardiac output. Reduced perfusion results in metabolic acidosis (a buildup of acid due to inadequate oxygen delivery to tissues), which further impairs cellular function.
Coronary perfusion also declines as blood pressure falls, potentially reducing myocardial contractility and worsening the situation. Without urgent drainage of pericardial fluid, typically via pericardiocentesis, tamponade progresses to obstructive shock, circulatory collapse, and cardiac arrest.
Clinical Connections
Cardiac tamponade presents with signs of obstructive shock caused by impaired ventricular filling. Hypotension, tachycardia, elevated jugular venous pressure, and muffled heart sounds form the classic constellation known as Beck’s triad, although all three features are not always present simultaneously. Early symptoms may include breathlessness due to reduced cardiac output and pulmonary congestion, chest discomfort from pericardial stretch, and marked anxiety related to sympathetic activation and falling perfusion. As haemodynamic compromise progresses, patients may develop altered level of consciousness, cool peripheries, and narrowing pulse pressure.
Certain clinical findings should immediately raise suspicion of tamponade physiology:
Rapidly falling blood pressure with persistent tachycardia despite fluid administration.
Rising jugular venous pressure with clear lung fields, suggesting obstructed venous return rather than primary left-sided failure.
Pulsus paradoxus, an exaggerated inspiratory drop in systolic blood pressure.
Echocardiography is considered the gold standard diagnostic modality because it visualises pericardial effusion and demonstrates diastolic collapse of the right atrium or right ventricle, indicating elevated intrapericardial pressure. It also helps assess chamber size, ventricular filling, and overall cardiac function. Once tamponade is identified, definitive treatment requires urgent removal of pericardial fluid, typically via pericardiocentesis under imaging guidance or surgical drainage when indicated. Prompt decompression restores ventricular filling and rapidly improves haemodynamics.
Ongoing monitoring remains essential after intervention. Re-accumulation of fluid, arrhythmias, bleeding, or persistent haemodynamic instability may occur. Continuous assessment of blood pressure, heart rate, jugular venous pressure, urine output, and symptom progression is critical to detect early deterioration. Timely recognition and coordinated emergency response are central to preventing progression to cardiovascular collapse.
Concept Check
Why is cardiac tamponade classified as a form of obstructive shock?
Why does rapid fluid accumulation cause tamponade more readily than slow accumulation?
Why are right-sided cardiac chambers affected first?
What mechanism produces pulsus paradoxus in tamponade?
Why does fluid resuscitation alone fail to correct tamponade?