Coagulation Studies
Coagulation studies assess the blood's ability to form and break down clots. They provide valuable information about the coagulation cascade, anticoagulant therapy and disorders that increase the risk of bleeding or thrombosis. These tests are commonly requested before surgery, when investigating unexplained bleeding or bruising, monitoring anticoagulant therapy, or assessing patients with liver disease, sepsis or disseminated intravascular coagulation (DIC).
Blood clotting is a complex process involving platelets, clotting factors and fibrinolysis. When any part of this system is disrupted, patients may experience excessive bleeding, inappropriate clot formation or both. Understanding coagulation results helps clinicians recognise these abnormalities and guide appropriate management.
What You Need to Know
Haemostasis occurs in three overlapping stages. First, platelets rapidly adhere to the damaged blood vessel to form a temporary platelet plug. Next, clotting factors activate the coagulation cascade, producing fibrin that stabilises the clot. Finally, once healing has occurred, the clot is gradually broken down by fibrinolysis.
Coagulation studies assess different parts of this process. Some tests measure how quickly a clot forms, while others assess clot breakdown or the number of circulating platelets. Looking at the overall pattern of results often provides far more information than interpreting a single test in isolation.
Many conditions can affect coagulation, including anticoagulant medications, liver disease, vitamin K deficiency, inherited clotting disorders, sepsis, trauma and massive haemorrhage. Understanding the patient's medications and clinical presentation is therefore essential when interpreting coagulation studies.
Key points:
Coagulation studies assess the body's ability to form and regulate blood clots.
They help investigate bleeding disorders, thrombotic disorders and monitor anticoagulant therapy.
Different tests assess different parts of the coagulation process.
Abnormal coagulation results do not always indicate spontaneous bleeding.
Coagulation studies should always be interpreted alongside platelet count, liver function tests and the patient's clinical presentation.
Patterns of abnormalities often provide greater diagnostic value than isolated results.
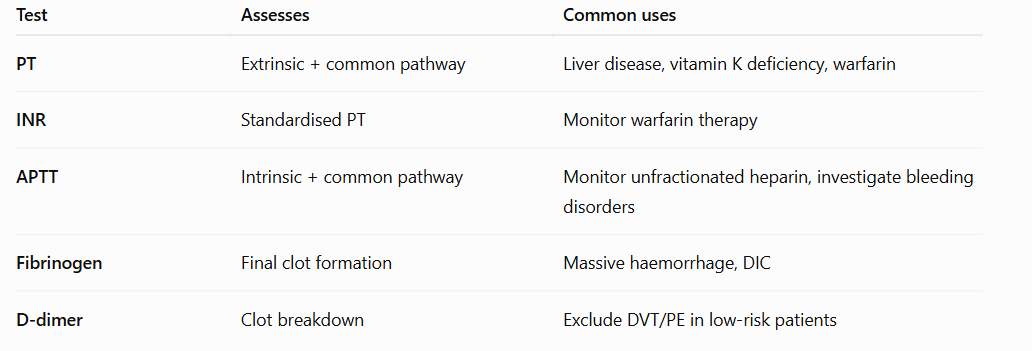
Components of Coagulation Studies:
International Normalised Ratio (INR)
Prothrombin Time (PT)
Activated Partial Thromboplastin Time (APTT)
Fibrinogen
D-dimer
Anti-Xa level
Thrombin Time (TT)
Beyond the Basics
International Normalised Ratio (INR)
Reference range
0.8–1.2 (patients not receiving anticoagulation)
The International Normalised Ratio (INR) is a standardised measure of the extrinsic coagulation pathway. It is calculated from the prothrombin time (PT) and allows results to be compared between laboratories. INR is primarily used to monitor warfarin therapy but also provides information about liver synthetic function and vitamin K-dependent clotting factors.
Decreased INR: A reduced INR indicates blood is clotting more quickly than expected. It may occur with inadequate warfarin therapy, increased vitamin K intake or laboratory variation. Mild reductions are rarely clinically significant.
Elevated INR: An increased INR indicates blood is taking longer to clot. Common causes include warfarin therapy, liver disease, vitamin K deficiency, disseminated intravascular coagulation (DIC) and deficiencies of clotting factors. As the INR rises, the risk of bleeding generally increases, particularly in patients receiving anticoagulants.
INR should always be interpreted within the clinical context. A patient with an INR of 3.0 taking warfarin for atrial fibrillation may be within their therapeutic range, whereas the same result in a patient not receiving anticoagulants is abnormal and requires investigation.
Prothrombin Time (PT)
Reference range
Approximately 11–15 seconds (varies between laboratories)
Prothrombin time measures how long it takes blood to clot via the extrinsic and common coagulation pathways. It is sensitive to deficiencies of vitamin K-dependent clotting factors and is the basis for calculating the INR.
Shortened PT: A shortened PT is uncommon and is generally not clinically significant.
Prolonged PT: A prolonged PT may occur with warfarin therapy, liver disease, vitamin K deficiency, DIC or deficiencies of clotting factors in the extrinsic pathway.
PT is most useful when interpreted alongside INR and APTT to help identify which part of the coagulation cascade is affected.
Activated Partial Thromboplastin Time (APTT)
Reference range
Approximately 25–35 seconds (varies between laboratories)
Activated partial thromboplastin time (APTT) measures the intrinsic and common coagulation pathways. It is commonly used to monitor unfractionated heparin therapy and investigate bleeding disorders involving intrinsic pathway clotting factors.
Shortened APTT: A shortened APTT is uncommon and usually has little clinical significance. It may occasionally occur in inflammatory states or with elevated clotting factor levels.
Prolonged APTT: A prolonged APTT commonly occurs with unfractionated heparin therapy, haemophilia, von Willebrand disease, liver disease, DIC and deficiencies of intrinsic pathway clotting factors.
Interpreting the APTT together with the PT helps narrow the differential diagnosis by identifying whether the intrinsic, extrinsic or common coagulation pathway is affected.
Fibrinogen
Reference range
2.0–4.0 g/L
Fibrinogen is a soluble plasma protein produced by the liver and is converted into fibrin during the final stages of coagulation. Fibrin forms the structural framework that stabilises the platelet plug and creates a durable blood clot.
Decreased fibrinogen: Reduced fibrinogen levels may occur with massive haemorrhage, disseminated intravascular coagulation (DIC), severe liver disease or congenital fibrinogen disorders. Low fibrinogen increases the risk of significant bleeding because insufficient fibrin is available to stabilise the clot.
Elevated fibrinogen: Increased fibrinogen commonly occurs during inflammation, infection, pregnancy, malignancy and other acute phase responses. Elevated levels may contribute to an increased risk of thrombosis.
Fibrinogen is particularly important in major trauma and obstetric haemorrhage, where it is often one of the earliest clotting factors to become critically depleted.
D-dimer
Reference range
<0.5 mg/L FEU (or laboratory equivalent)
D-dimer is a protein fragment produced when fibrin clots are broken down during fibrinolysis. Rather than indicating clot formation itself, D-dimer indicates that clot formation and subsequent clot breakdown have occurred somewhere within the body.
Decreased D-dimer: A normal D-dimer is useful because it makes significant thrombus formation unlikely in appropriately selected low-risk patients.
Elevated D-dimer: Increased D-dimer levels occur whenever significant clot formation and fibrinolysis are occurring. Common causes include deep vein thrombosis (DVT), pulmonary embolism (PE), disseminated intravascular coagulation (DIC), recent surgery, trauma, pregnancy, infection, malignancy and increasing age.
D-dimer is highly sensitive but poorly specific. An elevated result does not diagnose a thrombus and should never be interpreted in isolation. Instead, it should be interpreted alongside the patient's symptoms, clinical probability and imaging where appropriate. A normal D-dimer is often more clinically useful than an elevated one because it can help exclude venous thromboembolism in low-risk patients.
Anti-Xa Level
Reference range
Not routinely reported as a normal reference range. Therapeutic targets vary depending on the anticoagulant and indication.
Anti-Xa assays measure the activity of factor Xa inhibitors rather than the time taken for blood to clot. They are primarily used to monitor anticoagulant therapy with unfractionated heparin (UFH), low molecular weight heparin (LMWH) and, in selected circumstances, direct factor Xa inhibitors. Unlike the APTT, Anti-Xa directly measures the anticoagulant effect, making it a more reliable indicator in many clinical situations.
Decreased Anti-Xa: A low Anti-Xa level may indicate subtherapeutic anticoagulation due to inadequate dosing, delayed administration, poor absorption or increased drug clearance. Patients may remain at increased risk of thrombus formation if anticoagulation is insufficient.
Elevated Anti-Xa: An elevated Anti-Xa level indicates greater anticoagulant activity and may occur with excessive dosing, impaired renal function or drug accumulation. High levels increase the risk of bleeding and may require dose adjustment depending on the anticoagulant being monitored.
Anti-Xa results should always be interpreted alongside the patient's indication for anticoagulation, renal function, bleeding risk and timing of the blood sample relative to drug administration. Unlike INR or APTT, there is no single "normal" therapeutic Anti-Xa level because target ranges vary according to the anticoagulant being used.
Thrombin Time (TT)
Reference range
Approximately 14–21 seconds(varies between laboratories)
Thrombin time (TT) measures the final stage of coagulation by assessing how long it takes thrombin to convert fibrinogen into fibrin. Unlike PT and APTT, which assess multiple clotting factors within the coagulation cascade, TT specifically evaluates the final step of clot formation. It is particularly sensitive to abnormalities affecting fibrinogen and the presence of thrombin inhibitors.
Shortened TT: A shortened thrombin time is uncommon and is generally not considered clinically significant.
Prolonged TT: A prolonged thrombin time may occur with unfractionated heparin therapy, direct thrombin inhibitors, hypofibrinogenaemia, dysfibrinogenaemia, severe liver disease or disseminated intravascular coagulation (DIC). It may also be prolonged when fibrin degradation products interfere with normal clot formation.
Thrombin time is not routinely requested for most patients but is useful when investigating unexplained abnormalities in coagulation studies or assessing disorders affecting fibrinogen. TT should always be interpreted alongside fibrinogen, PT and APTT to help determine the underlying cause.
In Practice
Understanding what each coagulation test measures is only the first step. In clinical practice, coagulation studies are interpreted alongside the patient's history, medications, bleeding or thrombotic risk, physical examination and other investigations. The following scenarios demonstrate how patterns of abnormal coagulation results help identify underlying disorders and guide patient management.
Scenario 1: Supratherapeutic warfarin
A 79-year-old man taking warfarin for atrial fibrillation (AF) presents with spontaneous epistaxis and extensive bruising. He recently completed a course of antibiotics.
Coagulation studies
INR: 6.8
PT: 62 seconds
APTT: 44 seconds
Fibrinogen: 3.2 g/L
D-dimer: 0.3 mg/L FEU
Interpretation
The markedly elevated INR and prolonged PT indicate excessive anticoagulation due to warfarin. Antibiotics can potentiate the effects of warfarin by altering vitamin K production in the gut, increasing the risk of bleeding. This patient requires urgent assessment and reversal of anticoagulation based on the severity of bleeding.
Scenario 2: Deep vein thrombosis
A 63-year-old woman presents with unilateral calf swelling, pain and redness three days after a total knee replacement.
Coagulation studies
INR: 1.0
PT: 12 seconds
APTT: 30 seconds
Fibrinogen: 5.6 g/L
D-dimer: 3.4 mg/L FEU
Interpretation
Although the PT, INR and APTT are normal, the markedly elevated D-dimer indicates recent clot formation and breakdown. In the context of recent surgery and unilateral leg swelling, deep vein thrombosis should be strongly suspected. The diagnosis should be confirmed with appropriate imaging rather than D-dimer alone.
Scenario 3: Disseminated intravascular coagulation (DIC)
A 56-year-old patient with septic shock develops widespread bruising, bleeding from venepuncture sites and haemodynamic instability.
Coagulation studies
INR: 2.4
PT: 29 seconds
APTT: 71 seconds
Fibrinogen: 0.8 g/L
D-dimer: >20 mg/L FEU
Platelets: 42 × 10⁹/L
Interpretation
This pattern is highly suggestive of disseminated intravascular coagulation. Widespread activation of coagulation consumes clotting factors, fibrinogen and platelets while simultaneously producing large amounts of fibrin degradation products. DIC is a life-threatening emergency requiring treatment of the underlying cause together with supportive management of bleeding and coagulation abnormalities.
Scenario 4: Monitoring unfractionated heparin
A 67-year-old man is receiving an intravenous unfractionated heparin infusion following a pulmonary embolism.
Coagulation studies
INR: 1.1
PT: 13 seconds
APTT: 96 seconds
Anti-Xa: 0.82 IU/mL
Fibrinogen: 3.8 g/L
Interpretation
The prolonged APTT and therapeutic Anti-Xa level indicate that the heparin infusion is producing the intended anticoagulant effect. Anti-Xa monitoring is increasingly used because it provides a more direct assessment of heparin activity and is less affected by factors that may alter the APTT.
Scenario 5: Severe liver disease
A 61-year-old man with decompensated cirrhosis presents with increasing abdominal distension and easy bruising.
Coagulation studies
INR: 2.1
PT: 25 seconds
APTT: 48 seconds
Fibrinogen: 1.4 g/L
Thrombin time: 31 seconds
Interpretation
The prolonged PT, INR, APTT and thrombin time, together with reduced fibrinogen, indicate impaired production of clotting factors due to advanced liver disease. Because the liver synthesises most coagulation factors and fibrinogen, severe hepatic dysfunction can significantly impair haemostasis and increase the risk of bleeding, particularly during invasive procedures.