Liver Function Tests (LFTs)
Liver function tests (LFTs) are among the most commonly requested blood tests in healthcare. They provide valuable information about liver cell injury, bile flow, protein synthesis and the liver's ability to perform its many metabolic functions. LFTs can help identify a wide range of conditions, including hepatitis, biliary obstruction, fatty liver disease, alcohol-related liver disease and cirrhosis.
Despite their name, not all LFTs directly measure liver function. Some indicate liver cell injury, while others assess bile flow or the liver's ability to produce essential proteins. For this reason, individual results should always be interpreted together rather than in isolation.
What You Need to Know
The liver performs hundreds of essential functions, including metabolising nutrients, producing proteins and clotting factors, storing glycogen and vitamins, detoxifying harmful substances and producing bile to aid digestion. Because of these diverse roles, different liver diseases affect different components of the LFT profile. For example, hepatitis primarily damages liver cells, resulting in elevated ALT and AST, whereas gallstones blocking the bile ducts typically cause elevations in ALP and GGT. Chronic liver disease may eventually impair protein synthesis, resulting in reduced albumin and an elevated INR.
Rather than focusing on a single abnormal result, it is more useful to identify patterns across the entire LFT profile. The pattern of abnormalities often provides important clues about the underlying disease process and guides further investigation.
Many factors can influence LFTs, including alcohol consumption, medications, obesity, strenuous exercise, pregnancy and bone disease. Equally important is determining whether abnormal results represent an acute injury or chronic liver disease that has developed over time.
Key points:
LFTs assess liver cell injury, bile flow and liver synthetic function.
They can help identify hepatitis, biliary obstruction, fatty liver disease, alcohol-related liver disease and cirrhosis.
Not all abnormal LFTs indicate primary liver disease.
Patterns of abnormalities are often more informative than isolated results.
LFTs should always be interpreted alongside the patient's clinical presentation and other investigations.
Understanding how each component relates to the others improves clinical interpretation.
Components of Liver Function Tests:
Alanine Aminotransferase (ALT)
Aspartate Aminotransferase (AST)
Alkaline Phosphatase (ALP)
Gamma-Glutamyl Transferase (GGT)
Bilirubin
Albumin
Total Protein
Beyond the Basics
Alanine Aminotransferase (ALT)
Reference range
Male: <45 U/L
Female: <35 U/L
Alanine aminotransferase (ALT) is an enzyme found primarily within liver cells (hepatocytes). When these cells become damaged or inflamed, ALT leaks into the bloodstream, making it one of the most sensitive markers of liver cell injury. Because ALT is found predominantly in the liver, it is considered more liver-specific than AST.
Decreased ALT: Low ALT levels are generally not clinically significant and are rarely investigated. Occasionally, reduced levels may occur in advanced liver disease or vitamin B6 deficiency.
Elevated ALT: An increased ALT commonly occurs with viral hepatitis, non-alcoholic fatty liver disease (NAFLD), alcohol-related liver disease, medication-induced liver injury, autoimmune hepatitis and acute liver injury. Markedly elevated ALT levels often suggest acute hepatocellular damage.
ALT should always be interpreted alongside AST and the remainder of the LFT profile. An isolated ALT elevation often suggests hepatocellular injury, whereas simultaneous abnormalities in ALP and GGT may indicate mixed liver disease or cholestasis.
Aspartate Aminotransferase (AST)
Reference range
Male: <40 U/L
Female: <35 U/L
Aspartate aminotransferase (AST) is an enzyme found in the liver, cardiac muscle, skeletal muscle, kidneys and brain. Although AST rises following liver injury, it is less specific than ALT because damage to other tissues can also increase AST levels.
Decreased AST: Low AST levels are generally not clinically significant.
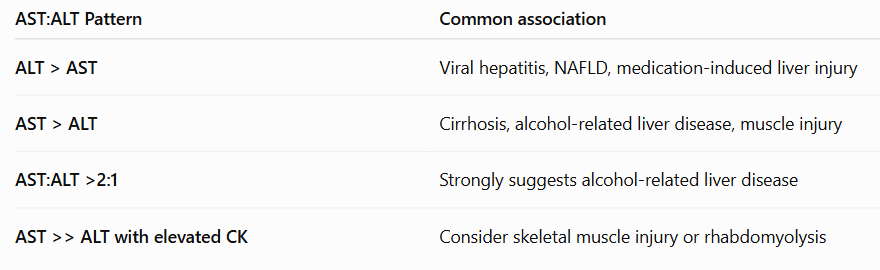
Elevated AST: Increased AST commonly occurs with hepatitis, alcohol-related liver disease, cirrhosis, muscle injury, strenuous exercise, myocardial infarction and certain medications. In alcohol-related liver disease, AST is often higher than ALT.
AST should never be interpreted alone. Because it is present in many tissues, elevated AST should always be considered alongside ALT, creatine kinase (CK) and the patient's clinical presentation.
AST:ALT Ratio
Alanine aminotransferase (ALT) and aspartate aminotransferase (AST) are both enzymes released into the bloodstream when liver cells are damaged. Comparing the ratio of AST to ALT can provide additional clues about the underlying cause of liver injury.
ALT greater than AST (AST:ALT ratio <1)
When ALT is higher than AST, the pattern is generally more consistent with hepatocellular injury. This is commonly seen in:
Acute viral hepatitis
Non-alcoholic fatty liver disease (NAFLD)
Medication-induced liver injury
Autoimmune hepatitis
Because ALT is found predominantly within the liver, it is considered more liver-specific than AST.
AST greater than ALT (AST:ALT ratio >1)
When AST is higher than ALT, several conditions should be considered. Mild elevations may occur with advanced fibrosis or cirrhosis, while more significant elevations are commonly associated with alcohol-related liver disease.
AST:ALT ratio greater than 2:1
An AST:ALT ratio of greater than 2:1 is strongly suggestive of alcohol-related liver disease, particularly when accompanied by an elevated GGT and a history of excessive alcohol consumption.
Several factors contribute to this pattern. Alcohol damages the mitochondria within liver cells, releasing mitochondrial AST into the bloodstream. Chronic alcohol use is also associated with vitamin B₆ deficiency, which reduces ALT production more than AST, further increasing the ratio.
Alkaline Phosphatase (ALP)
Reference range
30–120 U/L
Alkaline phosphatase (ALP) is an enzyme found predominantly in the liver and bones, with smaller amounts present in the intestine and placenta. Within the liver, ALP is concentrated in the bile ducts and is an important marker of cholestasis or biliary obstruction.
Decreased ALP: Reduced ALP levels are uncommon but may occur with malnutrition, zinc deficiency, hypothyroidism or rare inherited disorders such as hypophosphatasia.
Elevated ALP: Increased ALP commonly occurs with biliary obstruction, gallstones, cholangitis, primary biliary cholangitis, bone disorders, pregnancy and periods of rapid bone growth in children.
Because ALP is also produced by bone, it should always be interpreted alongside GGT. A raised ALP with a normal GGT suggests a bone source, whereas simultaneous elevation of both ALP and GGT is more suggestive of hepatobiliary disease.
Gamma-Glutamyl Transferase (GGT)
Reference range
Male: <60 U/L
Female: <40 U/L
Gamma-glutamyl transferase (GGT) is an enzyme found mainly in the liver and biliary tract. It is highly sensitive to hepatobiliary disease and is commonly used to determine whether an elevated ALP originates from the liver rather than bone.
Decreased GGT: Low GGT levels are not clinically significant.
Elevated GGT: Increased GGT commonly occurs with alcohol use, fatty liver disease, biliary obstruction, hepatitis and medications that induce liver enzymes. GGT is particularly sensitive but is not specific for liver disease.
GGT should almost always be interpreted together with ALP. An isolated GGT elevation may occur with alcohol consumption or certain medications, whereas simultaneous elevation of ALP and GGT strongly suggests hepatobiliary disease.
Bilirubin
Reference range
3–20 µmol/L
Bilirubin is a yellow pigment produced during the breakdown of haemoglobin from ageing red blood cells. The liver processes bilirubin before excreting it in bile. Elevated bilirubin may result from increased production, impaired liver processing or obstruction of bile flow.
Decreased bilirubin: Low bilirubin levels are not clinically significant.
Elevated bilirubin: Increased bilirubin commonly occurs with haemolysis (premature destruction of red blood cells), hepatitis, cirrhosis, biliary obstruction and inherited disorders such as Gilbert syndrome. Significant elevations may result in jaundice, dark urine and pale stools.
Bilirubin should always be interpreted alongside ALT, AST, ALP and GGT to determine whether the underlying cause is pre-hepatic, hepatic or post-hepatic.
Albumin
Reference range
35–50 g/L
Albumin is the most abundant protein in the blood and is produced exclusively by the liver. It helps maintain oncotic pressure (the ability of large plasma proteins, such as albumin, to pull water into the bloodstream) and transports hormones, medications and other substances throughout the body. Because albumin has a long half-life, it is a marker of chronic rather than acute liver function.
Decreased albumin: Reduced albumin commonly occurs with chronic liver disease, malnutrition, nephrotic syndrome, severe burns, protein-losing enteropathy and chronic inflammation. Patients may develop peripheral oedema or ascites due to reduced oncotic pressure.
Elevated albumin: Increased albumin is uncommon and is usually caused by dehydration rather than increased production.
Albumin should be interpreted alongside total protein, INR and the patient's nutritional and hydration status. A low albumin level does not necessarily indicate liver disease.
Total Protein
Reference range
60–80 g/L
Total protein measures the combined concentration of albumin and globulins within the blood. It provides a general assessment of protein status and may help identify liver disease, kidney disease, chronic inflammation or plasma cell disorders.
Decreased total protein: Reduced total protein may occur with chronic liver disease, malnutrition, nephrotic syndrome, severe burns or protein-losing enteropathy.
Elevated total protein: Increased total protein commonly occurs with dehydration, chronic inflammation, autoimmune disease and plasma cell disorders such as multiple myeloma.
Total protein should always be interpreted alongside albumin. Comparing these results helps determine whether abnormalities are due to changes in albumin, globulins or both, providing additional clues to the underlying condition.
In Practice
Understanding what each component of the LFT profile measures is only the first step. In clinical practice, liver function tests are interpreted alongside the patient's history, symptoms, medications, physical examination and other investigations. The following scenarios demonstrate how patterns of abnormal LFTs can help identify the underlying cause of liver dysfunction and guide further assessment and management.
Scenario 1: Acute viral hepatitis
A 23-year-old university student presents with fatigue, nausea, right upper quadrant pain and jaundice. He returned from overseas two weeks ago and reports dark urine and pale stools.
LFTs
ALT: 1,485 U/L
AST: 1,210 U/L
ALP: 102 U/L
GGT: 58 U/L
Bilirubin: 96 µmol/L
Albumin: 42 g/L
Total protein: 74 g/L
Interpretation
The markedly elevated ALT and AST indicate significant hepatocellular injury, while the elevated bilirubin explains the patient's jaundice. The relatively normal ALP suggests the primary problem is liver cell damage rather than biliary obstruction. This pattern is highly suggestive of acute viral hepatitis and should prompt hepatitis serology and further investigation.
Scenario 2: Gallstone causing biliary obstruction
A 58-year-old woman presents with severe right upper quadrant pain following a fatty meal. She is visibly jaundiced and reports dark urine and pale stools.
LFTs
ALT: 145 U/L
AST: 122 U/L
ALP: 412 U/L
GGT: 598 U/L
Bilirubin: 78 µmol/L
Albumin: 39 g/L
Total protein: 71 g/L
Interpretation
The marked elevation in ALP and GGT, together with an elevated bilirubin, indicates a cholestatic pattern of liver injury consistent with biliary obstruction. The mild elevation in ALT and AST suggests secondary liver cell irritation. In this patient, the clinical presentation is highly suggestive of choledocholithiasis (a gallstone obstructing the common bile duct).
Scenario 3: Alcohol-related liver disease
A 54-year-old man presents with increasing abdominal distension and fatigue. He reports drinking 10-12 standard drinks daily for many years.
LFTs
ALT: 68 U/L
AST: 156 U/L
ALP: 138 U/L
GGT: 612 U/L
Bilirubin: 34 µmol/L
Albumin: 29 g/L
Total protein: 64 g/L
Interpretation
The AST is more than twice the ALT, a pattern commonly associated with alcohol-related liver disease. The markedly elevated GGT further supports chronic alcohol use, while the reduced albumin suggests impaired liver synthetic function consistent with chronic liver disease or cirrhosis.
Scenario 4: Non-alcoholic fatty liver disease (NAFLD)
A 49-year-old woman with obesity and type 2 diabetes attends her GP for routine blood tests. She feels well and has no abdominal symptoms.
LFTs
ALT: 92 U/L
AST: 54 U/L
ALP: 96 U/L
GGT: 82 U/L
Bilirubin: 14 µmol/L
Albumin: 43 g/L
Total protein: 72 g/L
Interpretation
The mildly elevated ALT, with AST remaining lower than ALT, is a common pattern seen in non-alcoholic fatty liver disease. The slightly elevated GGT also supports hepatocellular injury. Normal bilirubin and albumin suggest preserved liver function despite ongoing liver inflammation.
Scenario 5: Bone disease rather than liver disease
A 71-year-old woman is being investigated for persistent back pain following a minor fall. She has no abdominal symptoms and denies alcohol use.
LFTs
ALT: 28 U/L
AST: 24 U/L
ALP: 368 U/L
GGT: 24 U/L
Bilirubin: 10 µmol/L
Albumin: 41 g/L
Total protein: 70 g/L
Interpretation
Although the ALP is markedly elevated, the normal GGT indicates the source is unlikely to be the liver. Because ALP is also produced by bone, this pattern is more suggestive of an underlying bone disorder such as a healing fracture, Paget's disease or bone metastases. This scenario highlights the importance of interpreting ALP alongside GGT rather than assuming all abnormal LFTs originate from the liver.