The Gastrointestinal Tract: Layers, Cellular Specialisation & Regional Adaptation
The gastrointestinal tract is not only specialised by region but also by its microscopic structure, which is precisely adapted to support digestion, absorption, secretion, and propulsion of contents. Despite the wide variety of functions performed from the oesophagus to the colon, the wall of the GI tract follows a consistent layered organisation. Within this shared framework, each region exhibits distinct histological modifications that reflect its specific physiological role.
What You Need to Know
Throughout most of the gastrointestinal tract, the wall follows a consistent structural plan made up of four primary layers: the mucosa, submucosa, muscularis externa, and either serosa or adventitia. Each layer contains specialised tissues and cell types that support digestion, secretion, motility, absorption, and protection. While this basic organisation is preserved from the oesophagus through to the large intestine, the relative thickness of each layer, the epithelial cell composition, and the degree of surface specialisation vary significantly depending on regional function.
This layered arrangement allows the gastrointestinal tract to perform multiple roles at the same time, rather than acting simply as a hollow tube for food passage. To understand how structure supports function, it is helpful to consider the key contributions of each layer:
the mucosa, which provides the interface for secretion, absorption, and barrier protection
the submucosa, which supports the mucosa structurally and houses blood vessels, lymphatics, and neural networks
the muscularis externa, which generates coordinated contractions for mixing and propulsion
the outer covering, either serosa or adventitia, which stabilises the organ within the abdominal cavity
Together, these layers allow the gastrointestinal tract to function as a digestive surface, a transport conduit, a defence barrier, and a neuromuscular control system. Regional adaptations in cell type, folding, and muscle arrangement ensure that each segment is structurally matched to its specific digestive role, supporting efficient processing of food while maintaining systemic homeostasis.
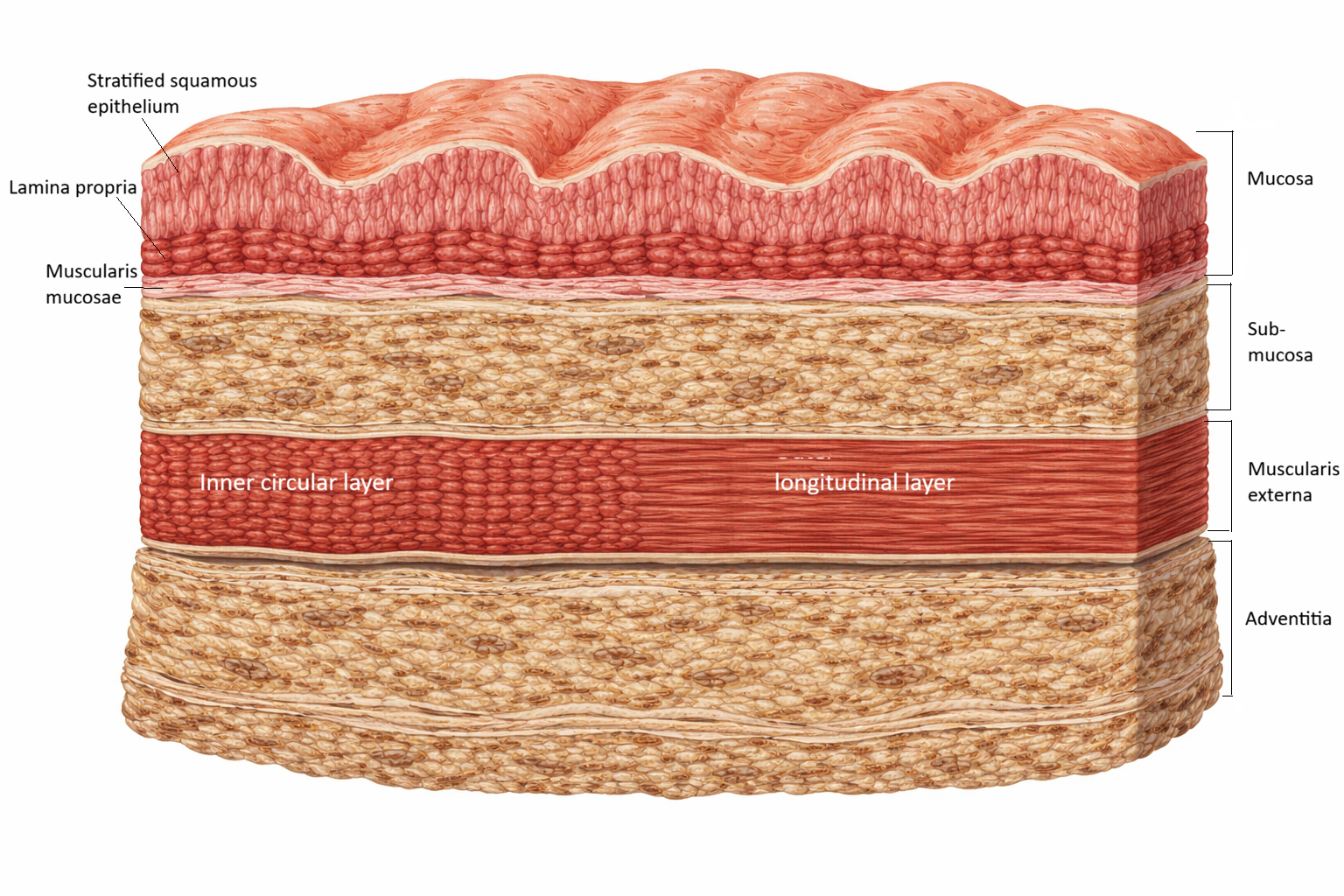
Image: Cross-section of the oesophageal wall showing the four structural layers: mucosa, submucosa, muscularis externa, and adventitia. The mucosa consists of stratified squamous epithelium, lamina propria, and muscularis mucosae. The muscularis externa contains an inner circular layer and an outer longitudinal layer, which work together to generate coordinated peristaltic movement.
Beyond the Basics
The Mucosa: Digestion, Absorption & Immune Defence
The mucosa is the innermost layer of the GI tract and is in direct contact with luminal contents. It consists of three sublayers: the epithelium, the lamina propria, and the muscularis mucosae. The epithelium is responsible for secretion, absorption, and barrier protection. In the oesophagus, it is composed of stratified squamous epithelium adapted for protection against mechanical abrasion. In the stomach and intestines, it transitions to simple columnar epithelium specialised for secretion and absorption.
The lamina propria is a loose connective tissue layer containing blood vessels, lymphatics, immune cells, and glands. It supports the epithelium metabolically and plays a critical role in immune surveillance through gut-associated lymphoid tissue. The muscularis mucosae is a thin smooth muscle layer that produces subtle local movements of the mucosa, enhancing contact between luminal contents and absorptive surfaces.
Together, these components allow the mucosa to carry out enzymatic secretion, nutrient uptake, immunological defence, and local surface mixing.
The Submucosa: Support, Secretion & Neural Control
The submucosa lies beneath the mucosa and consists of dense connective tissue that houses larger blood vessels, lymphatics, and submucosal glands. It provides structural support and flexibility while enabling rapid transport of absorbed nutrients into the systemic circulation.
Embedded within the submucosa is the submucosal (Meissner’s) plexus, a component of the enteric nervous system that regulates local blood flow, glandular secretion, and subtle muscularis mucosae activity. This neural network allows the digestive tract to adjust secretion and absorption independently of central nervous system input, while still being modulated by autonomic control.
The Muscularis Externa: Motility & Propulsion
The muscularis externa is responsible for the powerful contractile activity that propels contents along the digestive tract. It typically consists of an inner circular layer and an outer longitudinal layer of smooth muscle. Coordinated contraction and relaxation of these layers produce peristalsis, which moves contents forward, and segmentation, which mixes luminal contents with digestive secretions.
Between these muscle layers lies the myenteric (Auerbach’s) plexus, which regulates the strength, frequency, and coordination of smooth muscle contraction. This plexus is the primary controller of gastrointestinal motility and operates largely independently of central nervous system input.
Regional modifications occur within the muscularis externa. In the stomach, a third oblique muscle layer enhances mechanical mixing. In the colon, longitudinal muscle condenses into distinct bands known as taeniae coli, which contribute to haustral formation and slow transit for water absorption.
The Serosa & Adventitia: Protection & Anchoring
The outermost layer of the GI tract is either a serosa or an adventitia, depending on location. The serosa is a thin serous membrane that covers intraperitoneal organs, reducing friction between adjacent abdominal structures. It consists of simple squamous epithelium supported by connective tissue.
The adventitia is found in retroperitoneal structures, such as portions of the oesophagus and duodenum, and consists of connective tissue that anchors the organ to surrounding structures rather than allowing free movement.
Regional Histological Specialisation
Each segment of the GI tract exhibits distinctive histological adaptations. The oesophagus is protective, with thick stratified squamous epithelium and skeletal-to-smooth muscle transition in its muscular layer. The stomach contains gastric glands with specialised secretory cells, including parietal cells (acid and intrinsic factor secretion), chief cells (pepsinogen secretion), and mucous cells (protective mucus production).
The small intestine is structurally optimised for absorption. It displays large circular folds known as plicae circulares, along with villi and microvilli that massively increase surface area. The duodenum contains Brunner’s glands in the submucosa that secrete alkaline mucus to neutralise gastric acid. The ileum contains Peyer’s patches, which provide immune surveillance.
The large intestine lacks villi and is dominated by goblet cells that secrete mucus to facilitate waste passage. Its smooth muscle organisation promotes slow transit and efficient water absorption.
Barrier Function & Immune Defence
The GI epithelium forms one of the largest barrier surfaces in the body. Tight junctions between epithelial cells prevent uncontrolled movement of pathogens while allowing selective nutrient absorption. The lamina propria contains a dense population of immune cells that respond to microbial threats without provoking excessive inflammation.
This complex barrier function explains why disruption of mucosal integrity, as occurs in inflammatory bowel disease, chemotherapy, or severe infection, leads to profound systemic illness.
Clinical Connections
Many gastrointestinal disorders originate at the histological level, where disruption of normal cellular structure leads directly to functional impairment. Because each layer of the gastrointestinal wall performs a specific role, disease processes tend to produce predictable patterns of dysfunction involving absorption, secretion, motility, or immune defence.
Damage to the mucosa and underlying layers commonly alters digestion and nutrient uptake. In peptic ulcer disease, erosion of the gastric mucosa and submucosa compromises the protective barrier against acid, increasing the risk of bleeding and perforation. In coeliac disease, immune-mediated destruction of intestinal villi markedly reduces absorptive surface area, leading to malnutrition, weight loss, and micronutrient deficiencies despite adequate dietary intake.
Inflammatory bowel diseases extend beyond the mucosa to involve the full thickness of the intestinal wall. This transmural or extensive inflammation disrupts epithelial barrier integrity, alters smooth muscle function, and interferes with coordinated motility, contributing to symptoms such as diarrhoea, pain, strictures, and systemic inflammation. At a cellular level, these changes explain why inflammation in these conditions produces both local and extra-intestinal manifestations.
Histological change also underpins malignant transformation within the gastrointestinal tract. In chronic reflux disease, repeated injury to oesophageal epithelium promotes metaplastic change, predisposing to Barrett’s oesophagus and increasing the risk of adenocarcinoma. In the colon, altered epithelial turnover, glandular architecture, and dysregulated cell proliferation form the basis of colorectal cancer development.
Key clinical implications of gastrointestinal histology include:
reduced nutrient absorption when villi, microvilli, or epithelial integrity are compromised
impaired barrier function leading to inflammation, infection, or bleeding
altered motility resulting from smooth muscle or enteric nerve involvement
increased malignancy risk associated with chronic epithelial injury and abnormal cell turnover
Findings from gastrointestinal histology allows clinicians to link microscopic changes to clinical presentation and disease progression.
Concept Check
Why does most of the GI tract share a four-layered wall structure?
How does the mucosa differ between the oesophagus, stomach, and small intestine?
Why is the muscularis externa organised into circular and longitudinal layers?
Why does the small intestine possess villi while the large intestine does not?
How does the enteric nervous system integrate with GI histology to regulate function?