Organisation of the Gastrointestinal Tract & Accessory Organs
The digestive system is a highly coordinated organ system responsible for the ingestion, mechanical and chemical breakdown of food, absorption of nutrients and water, and elimination of waste. While digestion appears continuous, it is actually divided into specialised regional functions along the gastrointestinal (GI) tract, supported by a group of powerful accessory organs. Each segment of the digestive system is structurally adapted to its specific role, and disruption at any level can significantly impair digestion, absorption, metabolism, and overall homeostasis.
What You Need to Know
The gastrointestinal (GI) tract is a continuous, hollow muscular tube that extends from the mouth to the anus and is responsible for the ingestion, digestion, absorption, and elimination of nutrients. It includes the oral cavity, pharynx, oesophagus, stomach, small intestine, and large intestine, each structurally specialised to perform distinct but coordinated roles. While food physically passes through this tract, effective digestion depends on the accessory digestive organs, which release secretions that chemically break down food and create the conditions required for absorption.
Although these structures differ in form and function, they operate as an integrated system designed to maximise contact between food, digestive enzymes, and absorptive surfaces. This organisation allows digestion to progress in a controlled, stepwise manner rather than occurring all at once. To understand how this system functions as a whole, it is helpful to consider the key components involved in digestion and absorption:
The gastrointestinal tract, which provides the physical pathway for food movement and contains the muscular and mucosal layers required for mixing, propulsion, and absorption
The accessory organs, including the salivary glands, liver, gallbladder, and pancreas, which secrete enzymes, bile, and buffers but do not directly transport food
The regulatory systems, particularly smooth muscle activity and the enteric nervous system, which coordinate motility and secretion along the tract
Together, these elements allow the GI tract to regulate the rate at which food moves, ensure adequate mixing with digestive secretions, and optimise nutrient absorption. Although the enteric nervous system can function independently, it remains closely connected to the central nervous system, allowing digestion to adapt to factors such as stress, illness, and overall metabolic demand.
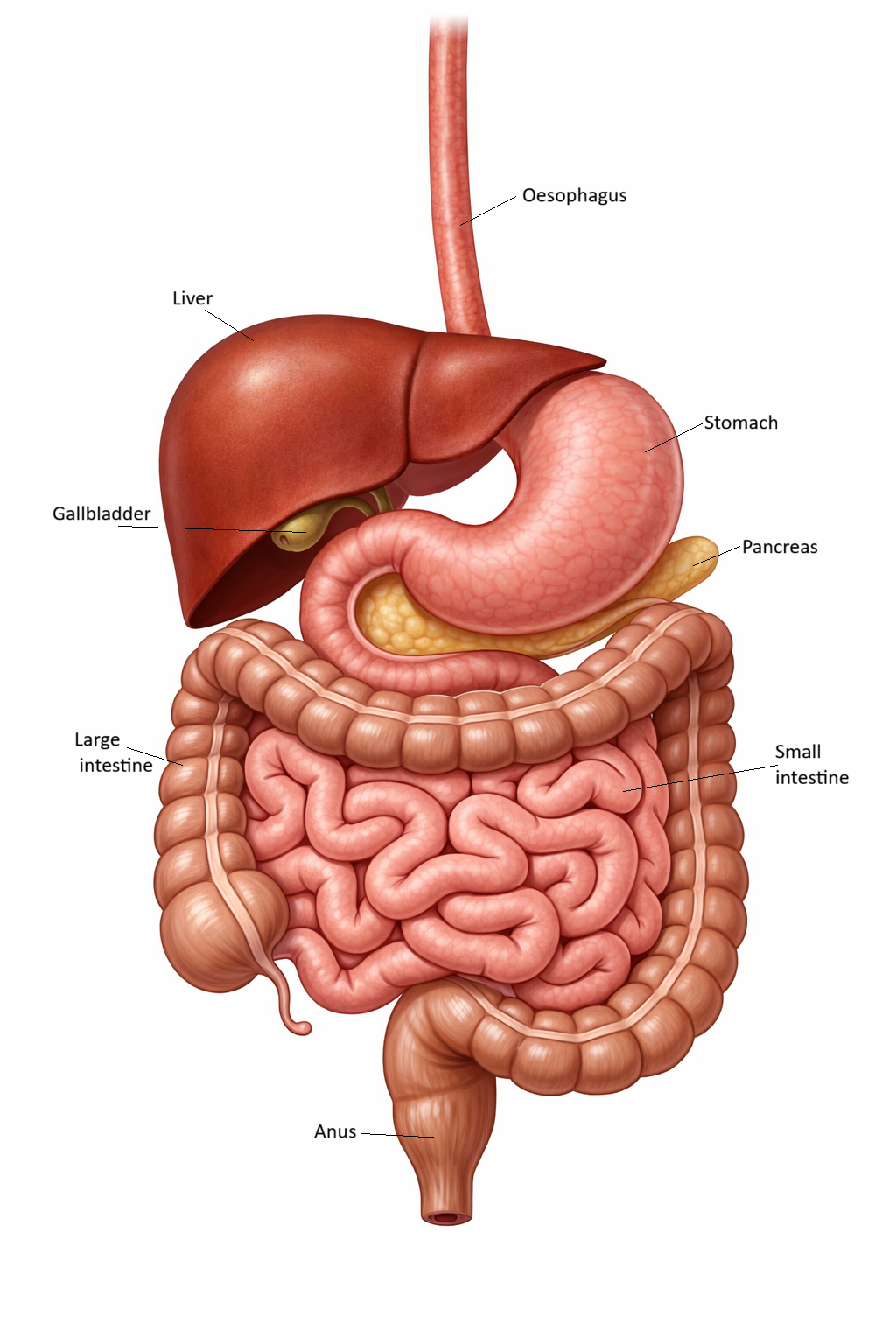
Image: Major abdominal organs of the gastrointestinal tract from oesophagus to rectum.
Beyond the Basics
The oral cavity and pharynx
Digestion begins in the oral cavity through a combination of mechanical and chemical processes that prepare food for safe swallowing and downstream digestion. Mastication (chewing) breaks food into smaller particles, increasing surface area for enzyme activity, while saliva moistens and binds food into a cohesive bolus. Salivary amylase (an enzyme produced by the salivary glands, mainly the parotid gland initiates carbohydrate digestion, although its activity is limited by the short time food remains in the mouth.
The pharynx functions as a shared pathway between the respiratory and digestive systems, requiring precise coordination to prevent airway compromise. Swallowing is initiated voluntarily but quickly transitions into an involuntary reflex, ensuring food is directed into the oesophagus while the airway is protected. This integration highlights the close relationship between digestion, respiration, and neuromuscular control.
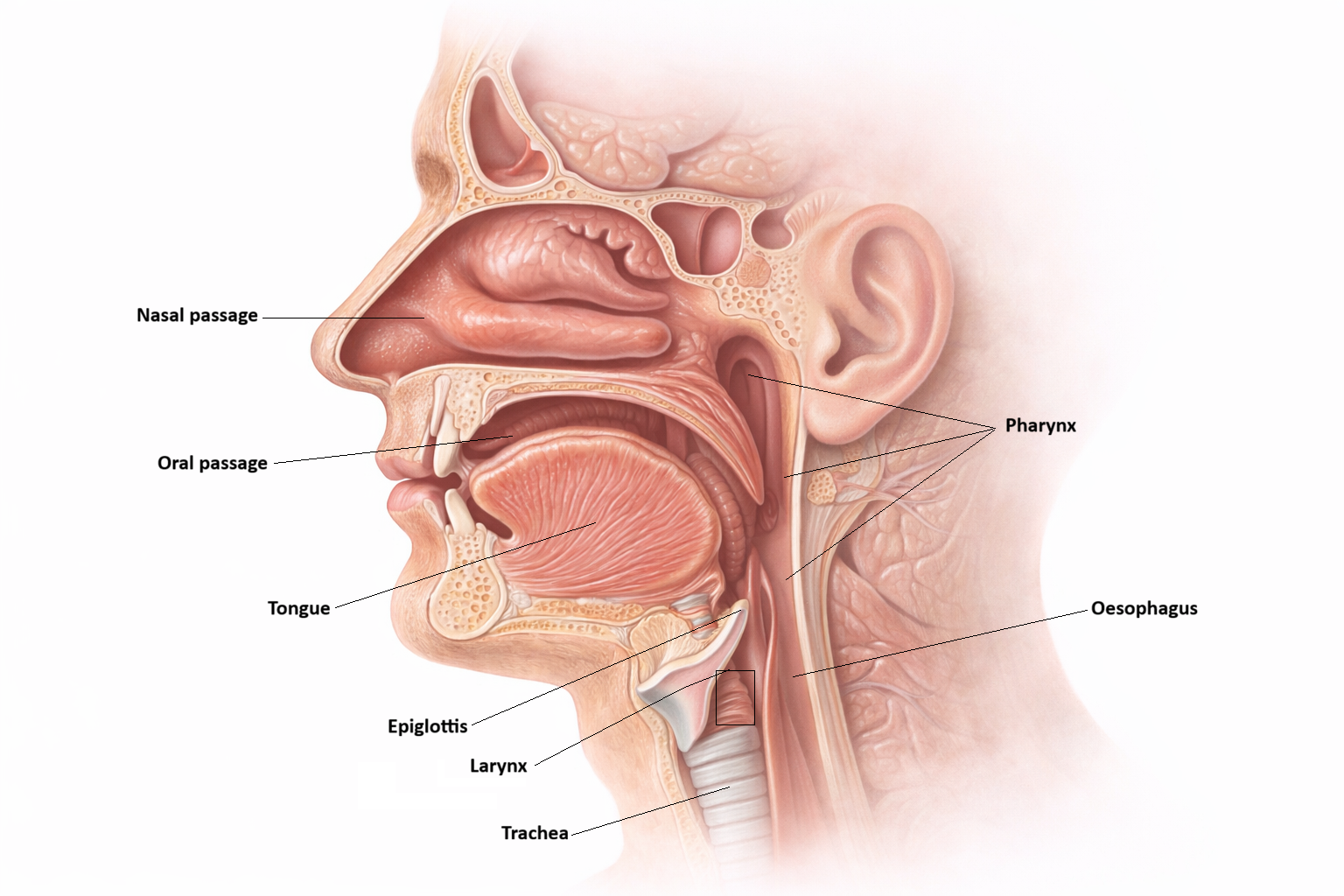
Image: The gastrointestinal tract begins at the mouth. Digestion is initiated here through mechanical breakdown by teeth and chemical action from saliva, before the food travels to the oesophagus.
The oesophagus
The oesophagus serves as a transport conduit rather than a site of digestion or absorption, moving food efficiently from the pharynx to the stomach. Peristaltic waves propel the bolus downward, independent of gravity, allowing swallowing to occur in a variety of body positions.
The presence of upper and lower oesophageal sphincters ensures unidirectional movement of food. The gradual transition from skeletal to smooth muscle along its length reflects the shift from voluntary initiation of swallowing to involuntary control as food approaches the stomach.
The wall of the oesophagus is organised into four distinct layers, each contributing to its structure and function. The innermost layer, the mucosa, consists of a stratified squamous epithelium that protects against abrasion from swallowed food, supported by a connective tissue lamina propria and a thin layer of smooth muscle known as the muscularis mucosae. Beneath this lies the submucosa, which contains connective tissue, blood vessels, and mucus-secreting glands that help lubricate the lumen. The muscularis externa is responsible for propulsion of food and is composed of two layers of muscle, an inner circular layer and an outer longitudinal layer, with a unique transition from skeletal muscle in the upper third to smooth muscle in the lower third, allowing both voluntary initiation and involuntary continuation of swallowing. The outermost layer is the adventitia, a connective tissue layer that anchors the oesophagus to surrounding structures, as it lacks a true serosal covering along most of its length.
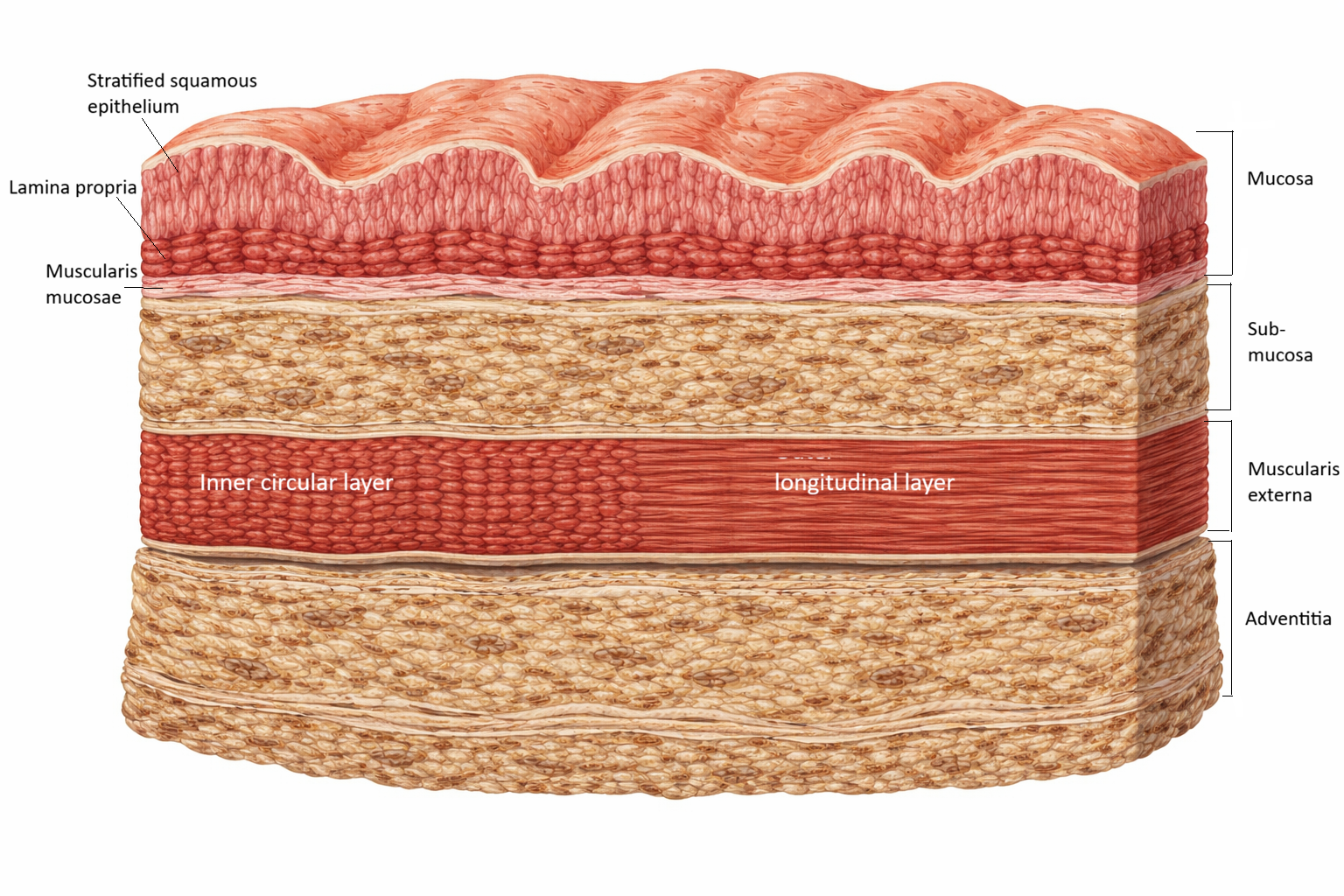
Image: Cross-section of the oesophageal wall showing the four structural layers: mucosa, submucosa, muscularis externa, and adventitia. The mucosa consists of stratified squamous epithelium, lamina propria, and muscularis mucosae. The muscularis externa contains an inner circular layer and an outer longitudinal layer, which work together to generate coordinated peristaltic movement.
The stomach
The stomach acts as both a temporary storage organ and a powerful mechanical mixer. Its muscular walls churn ingested food, blending it with gastric secretions to form chyme, a semi-liquid mixture optimised for controlled delivery into the small intestine.
Chemical digestion within the stomach focuses primarily on proteins. Hydrochloric acid denatures protein structure and activates pepsin from its inactive precursor, pepsinogen, while also providing antimicrobial protection. Intrinsic factor, secreted by parietal cells, is essential for vitamin B₁₂ absorption later in the digestive process, linking gastric function to haematological and neurological health.
The small intestine
The small intestine is the principal site of digestion and absorption, structurally adapted to maximise efficiency. In the duodenum, acidic chyme is neutralised by bicarbonate, creating an optimal pH for pancreatic enzymes and bile to act on fats, proteins, and carbohydrates.
As chyme moves into the jejunum, extensive mucosal folding and microscopic surface projections dramatically increase absorptive capacity. The ileum continues absorption while playing a specialised role in reclaiming bile salts and vitamin B₁₂, allowing these components to be recycled and reused. Together, these adaptations support efficient nutrient transfer into both the bloodstream and lymphatic system.
The large intestine
The large intestine is specialised for water and electrolyte recovery rather than nutrient digestion. Slower transit allows for maximal fluid absorption and compaction of waste material into faeces, supporting fluid balance and waste elimination.
Resident gut microbiota contribute to digestive health by fermenting undigested carbohydrates and producing short-chain fatty acids that nourish colonic cells. Although structurally simpler than the small intestine, the large intestine plays a critical role in maintaining metabolic and immune homeostasis.
Accessory digestive organs
The liver, gallbladder, and pancreas support digestion through tightly regulated secretory functions. The liver produces bile, which emulsifies dietary fats, while also processing absorbed nutrients, synthesising proteins, and detoxifying substances absorbed from the gut.
The gallbladder concentrates and stores bile between meals, releasing it into the duodenum in response to fat intake. The pancreas provides a broad spectrum of digestive enzymes alongside bicarbonate, which neutralises gastric acid and protects the intestinal mucosa. This coordinated secretion ensures digestion occurs efficiently without damaging intestinal tissue.
Functional integration of digestion
Digestion depends on the seamless integration of mechanical breakdown, chemical digestion, motility, and regulation. Each segment of the gastrointestinal tract is structurally adapted to perform specific tasks while remaining responsive to signals from neighbouring organs.
This coordination is governed by the enteric nervous system, autonomic input, and gastrointestinal hormones, allowing digestion to adapt to meal composition, volume, and physiological demand. Rather than functioning as isolated organs, the components of the digestive system operate as a unified and responsive network.
Clinical Connections
Disruption at any point along the gastrointestinal pathway can produce consequences that extend well beyond the digestive system itself. Because digestion, absorption, and fluid regulation occur in a sequential and interdependent manner, dysfunction in one region often leads to downstream nutritional, metabolic, and electrolyte disturbances.
Impairment of upper gastrointestinal structures commonly alters both nutrient processing and patient comfort. For example, oesophageal sphincter dysfunction allows reflux of acidic gastric contents into the oesophagus, increasing the risk of mucosal injury and aspiration. Disorders affecting the stomach interfere with protein digestion and intrinsic factor secretion, which can ultimately impair vitamin B₁₂ absorption and contribute to anaemia and neurological dysfunction.
Disorders of the intestines often have the most profound impact on nutritional status, as this is where the majority of absorption occurs. Small intestinal disease can rapidly lead to malnutrition, electrolyte imbalance, and dehydration, while pathology affecting the colon primarily disrupts fluid and electrolyte recovery and normal waste elimination. In clinical practice, this pattern of dysfunction is often reflected in changes to stool volume, consistency, and frequency, as well as abnormal laboratory findings.
Common clinical consequences associated with gastrointestinal dysfunction include:
malnutrition resulting from impaired digestion or absorption of macronutrients and micronutrients
dehydration and electrolyte imbalance due to altered fluid handling in the small or large intestine
reflux, aspiration risk, or oesophageal injury related to sphincter dysfunction
impaired vitamin B₁₂ absorption with associated haematological and neurological effects
Liver and pancreatic dysfunction produce particularly wide-ranging effects, as these organs are central to metabolic regulation as well as digestion. Reduced bile production or delivery impairs fat absorption and fat-soluble vitamin uptake, while pancreatic enzyme deficiency limits digestion of all major nutrient classes. Because the liver also regulates glucose storage, protein synthesis, and detoxification, disease in these organs frequently presents with systemic manifestations that require multidisciplinary assessment and management.
Concept Check
Why is the small intestine structurally specialised for absorption rather than the stomach?
How do the liver and pancreas support digestion without directly contacting food?
Why must chyme enter the duodenum slowly from the stomach?
Why does the large intestine prioritise water absorption rather than digestion?
How does disruption of bile secretion affect fat absorption?