LYMPHATIC VESSEL ANATOMY & LYMPH FLOW
The lymphatic system forms a vast, low-pressure network of vessels that collect excess fluid from tissues, filter it through lymph nodes and return it to the bloodstream. Without this system, the body would rapidly accumulate interstitial fluid, leading to severe oedema and impaired immune surveillance. Lymphatic vessels work alongside the cardiovascular system but operate very differently: they are one-way pathways that begin in tissues and end at the venous circulation.
What You Need to Know
Lymphatic vessel anatomy is designed to support slow, one-way movement of lymph from tissues back to the bloodstream. The system begins with lymphatic capillaries, which are microscopic, blind-ended vessels embedded throughout most tissues. These capillaries collect excess interstitial fluid, plasma proteins and cellular debris that escape from blood capillaries during normal circulation. Once inside the lymphatic system, this fluid is called lymph and becomes part of a regulated transport network rather than a passive overflow system.
As lymphatic capillaries converge, they form progressively larger vessels with a more defined structure. These collecting vessels contain numerous valves that enforce unidirectional flow and prevent lymph from moving backward under gravity or pressure changes. Several mechanisms work together to move lymph through this low-pressure system:
Contraction of surrounding skeletal muscles during movement
Changes in thoracic pressure during breathing
Rhythmic contraction of smooth muscle within lymphatic vessel walls
Pulsation of nearby arteries
These forces allow lymph to move steadily despite the absence of a central pump, making lymph flow highly dependent on movement and normal respiratory function.
As lymph travels centrally, it passes through lymph nodes positioned along predictable anatomical routes, where it is filtered and monitored before continuing onward. Ultimately, lymph from most of the body drains into the thoracic duct, while lymph from the upper right quadrant drains into the right lymphatic duct. Both ducts return lymph to the venous circulation near the subclavian veins. This completes the circuit, restoring fluid, proteins and immune cells to the bloodstream while maintaining tissue fluid balance and supporting immune surveillance.
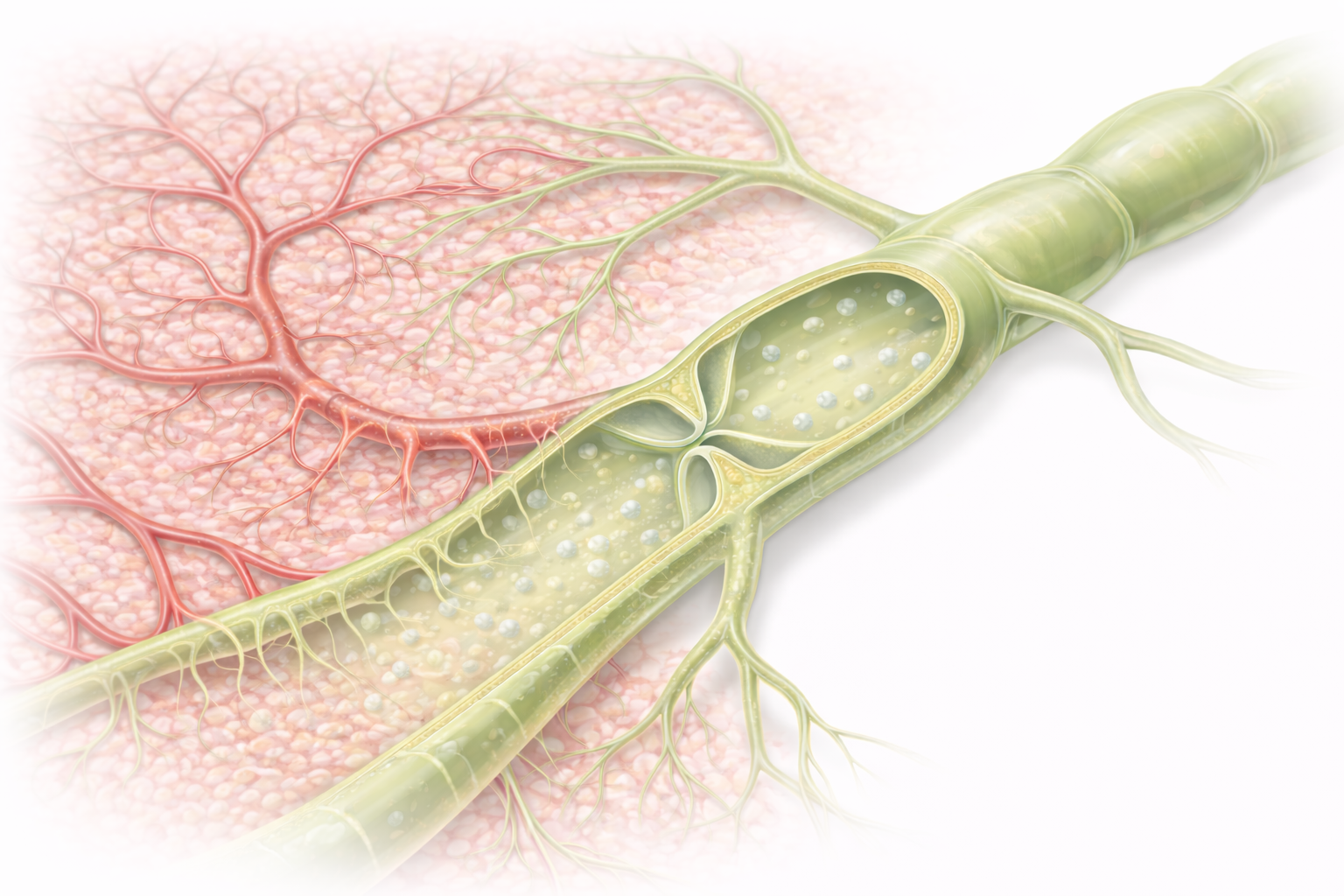
Image: Lymphatic capillaries begin as blind-ended vessels within tissues, where excess interstitial fluid from surrounding blood capillaries enters through overlapping endothelial flaps. These small capillaries merge into larger lymphatic vessels with valves, allowing lymph to move in a one-way direction back toward the circulation.
Beyond the Basics
Lymphatic Capillaries: Structural Sensitivity to Tissue Fluid
Lymphatic capillaries form the entry point of the lymphatic system and are uniquely adapted to respond to changes in tissue pressure. They are blind-ended microscopic vessels present in nearly all tissues, embedded within the interstitial space. Their walls consist of a single layer of endothelial cells arranged with overlapping edges. These overlaps function as one-way flaps that respond dynamically to pressure gradients rather than active control.
When interstitial pressure rises, such as during increased capillary filtration or inflammation, the endothelial flaps separate slightly, allowing fluid, plasma proteins, cellular debris and immune cells to enter the capillary lumen. As lymph accumulates and internal pressure increases, the flaps close, preventing backflow into tissues. This pressure-sensitive design allows lymphatic capillaries to act as highly responsive regulators of tissue fluid balance rather than passive drainage channels.
Collecting Vessels and Directional Flow Control
As lymphatic capillaries merge, they form collecting lymphatic vessels with a more defined wall structure. These vessels contain a thin layer of smooth muscle and numerous one-way valves, giving them a segmented appearance. The valves divide the vessels into functional units that ensure lymph moves only toward the central circulation, even against gravity.
Smooth muscle within the vessel wall contracts rhythmically, a process known as lymphangiomotor activity. This intrinsic pumping mechanism works continuously but generates only low pressure. Effective lymph transport therefore depends heavily on external forces that intermittently compress the vessels and drive lymph forward through the valves. These forces include skeletal muscle contraction during movement, arterial pulsation from adjacent vessels, changes in thoracic pressure during breathing, and general body movement. In combination, these mechanisms maintain steady lymph flow despite the absence of a central pump.
Lymphatic Trunks and Final Return to Circulation
Collecting vessels converge into larger lymphatic trunks that drain broad anatomical regions. These trunks act as conduits rather than filtration sites and channel lymph toward the major ducts. Ultimately, lymph enters either the thoracic duct or the right lymphatic duct, depending on its region of origin. These ducts represent the final stage of lymphatic transport and empty directly into the venous circulation at the subclavian veins.
The thoracic duct drains lymph from the lower body, abdomen, left thorax, left upper limb and left side of the head and neck, while the right lymphatic duct drains the upper right quadrant of the body. Together, they return several litres of lymph to the bloodstream each day, restoring plasma volume and maintaining circulatory stability.
Composition of Lymph and Regional Variation
Lymph composition reflects the tissue it drains. In most peripheral tissues, lymph is similar to interstitial fluid and contains water, plasma proteins, electrolytes and immune cells. In the small intestine, lymph is rich in absorbed lipids and is known as chyle. Its milky appearance is due to the presence of chylomicrons, large lipid transport particles that cannot enter blood capillaries directly. Variations in lymph composition provide insight into local tissue activity, metabolic processes and immune responses.
Regulation of Lymph Flow
Lymph flow is not constant and adapts to physiological demand. It increases when interstitial pressure rises, during inflammation, with increased capillary filtration and during physical activity or deep breathing. These conditions enhance both fluid entry into lymphatic capillaries and propulsion through collecting vessels. In contrast, lymph flow slows during immobility, lymphatic obstruction or vessel damage. Reduced flow increases the risk of fluid accumulation, impaired immune surveillance and infection, highlighting the dependence of lymphatic function on both structural integrity and normal movement.
Clinical Connections
Damage or obstruction of lymphatic vessels disrupts normal lymph flow and can lead to lymphoedema, a chronic condition characterised by persistent swelling, skin thickening and increased infection risk. This most commonly occurs after lymph node removal or radiotherapy in cancer treatment, where normal drainage pathways are interrupted. In some regions of the world, parasitic infections such as lymphatic filariasis cause progressive lymphatic damage, producing severe and disabling swelling over time.
Impaired lymphatic flow also affects immune function. Lymph is the transport medium for antigens, immune cells and inflammatory mediators moving from tissues to lymph nodes. When this movement is reduced or blocked, immune surveillance becomes less efficient, increasing susceptibility to infection and delaying resolution of inflammation. Recurrent cellulitis is a common complication in individuals with chronic lymphoedema, further worsening lymphatic dysfunction.
Clinical situations where lymphatic anatomy directly guides care include:
Predicting post-operative oedema following lymph node dissection
Identifying lymphatic involvement during infection or malignancy
Guiding manual lymphatic drainage techniques
Interpreting patterns of lymphadenopathy in local versus systemic disease
Assessment of limb swelling, skin integrity and lymph node changes provides important information about underlying lymphatic function. Accurate interpretation of these findings helps guide patient education, infection prevention strategies and escalation of care when lymphatic insufficiency progresses.
Concept Check
How do lymphatic capillaries allow fluid to enter while preventing backflow?
Why do lymphatic vessels require valves, and how do they contribute to lymph movement?
What role do skeletal muscles and breathing play in lymph transport?
Which regions of the body drain into the thoracic duct versus the right lymphatic duct?
What is chyle, and where does it form?