Neck of Femur (NOF) Fractures
Neck of femur fracture refers to a fracture occurring in the proximal femur, most commonly in older adults following a low-energy fall. Although often grouped under the broad term “hip fracture,” NOF fractures represent a distinct clinical entity due to their relationship with femoral head blood supply, immobility-related complications, and high associated morbidity and mortality. Understanding the pathophysiology of NOF fractures explains why they are managed urgently, why surgical approach depends on fracture location, and why outcomes are influenced by systemic factors as much as by the fracture itself.
What You Need to Know
Neck of femur fractures occur at a biomechanically critical junction between the femoral head and shaft, where forces from body weight and movement are transmitted from the pelvis to the lower limb. In many cases, the underlying bone is already weakened by osteoporosis, meaning that low-energy mechanisms such as a fall from standing height are sufficient to cause fracture. The combination of reduced bone strength and high mechanical demand explains why these injuries are common in older adults and why the fracture itself often represents only one part of a much broader physiological event.
These fractures are classified as intracapsular or extracapsular based on their relationship to the hip joint capsule. This distinction is clinically important because the femoral head relies on a limited vascular supply that is vulnerable to disruption, particularly in intracapsular fractures. When blood flow is compromised, bone healing is impaired and the risk of avascular necrosis increases. Extracapsular fractures generally preserve femoral head perfusion but introduce different challenges related to fracture stability and mechanical fixation.
Several key features shape the early clinical course and downstream consequences of a neck of femur fracture:
Intracapsular fractures place the femoral head blood supply at risk, affecting healing potential and surgical decision-making
Extracapsular fractures tend to bleed more due to their location outside the capsule, contributing to physiological stress
Sudden loss of mobility triggers systemic effects, including pain, stress response activation, and increased risk of complications
Beyond the local injury, neck of femur fractures rapidly initiate a cascade of systemic stressors. Acute pain, immobility and blood loss contribute to sympathetic activation, inflammatory response and metabolic demand. Prolonged immobility further increases the risk of complications such as thromboembolism, pneumonia and pressure injury. For this reason, neck of femur fractures are managed as both an orthopaedic emergency and a condition with significant whole-body consequences, rather than as an isolated skeletal injury.
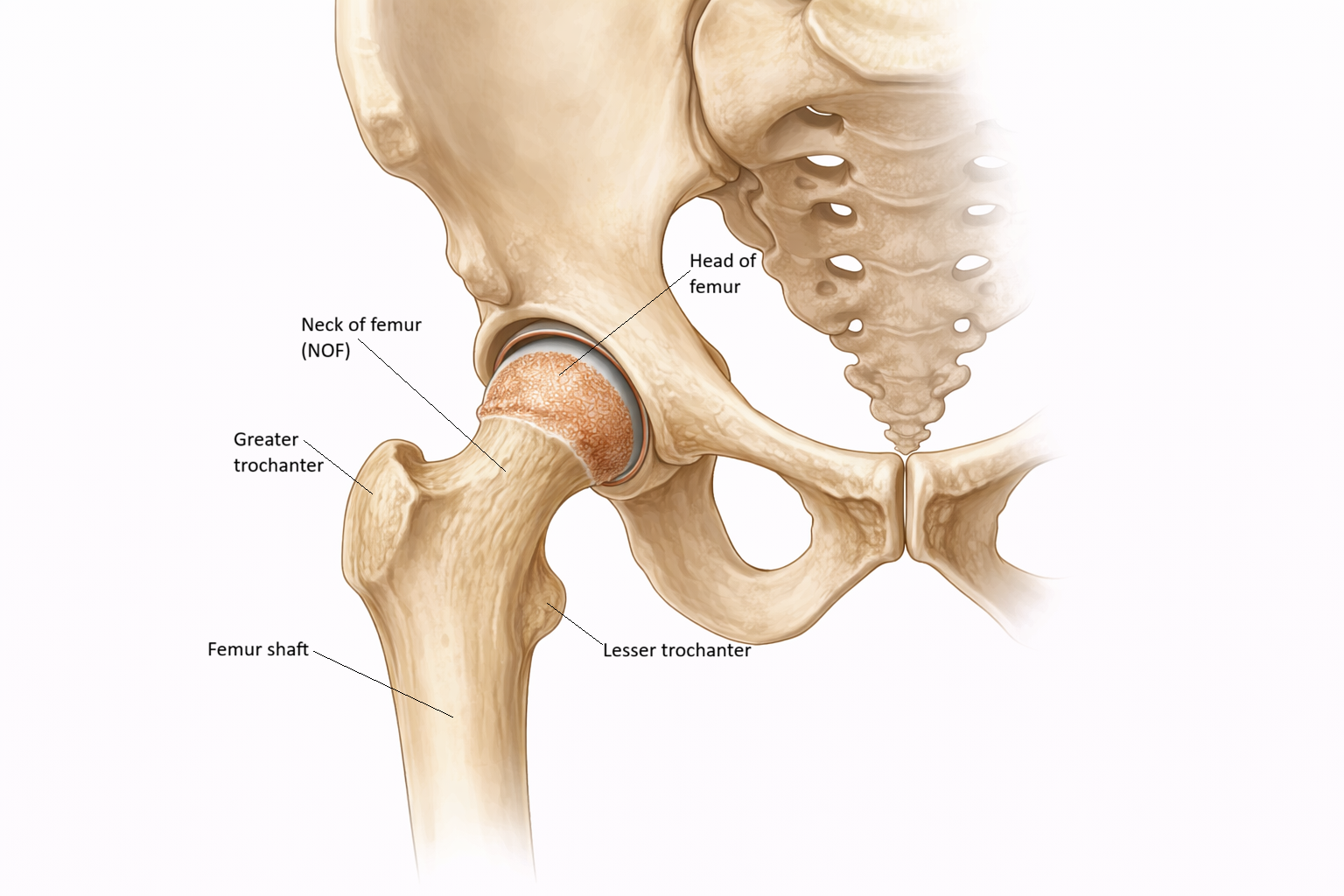
Image: The neck of femur is the narrow region between the femoral head and shaft, sitting within the hip joint where the head articulates with the acetabulum of the pelvis. This location is clinically important, as fractures here can disrupt blood supply to the femoral head and impair healing.
Beyond the Basics
Intracapsular vs extracapsular fractures
Intracapsular fractures occur within the hip joint capsule and include subcapital and transcervical fractures. Because these fractures lie inside the capsule, they directly endanger the blood vessels that supply the femoral head. These vessels run along the femoral neck within the joint capsule and are vulnerable to tearing, compression or kinking at the time of fracture. When blood flow is disrupted, the ability of bone cells to survive and repair is significantly reduced, increasing the risk of non-union and avascular necrosis.
Extracapsular fractures occur outside the joint capsule and include intertrochanteric and subtrochanteric fractures. In these injuries, blood supply to the femoral head is usually preserved because the intracapsular vessels remain intact. Healing potential is therefore more reliable, but extracapsular fractures often involve greater soft tissue disruption and bleeding. This occurs because the fracture site lies in a highly vascular region with more muscle attachment and less containment of bleeding.
Blood supply and avascular necrosis
The femoral head receives most of its blood supply from branches of the medial femoral circumflex artery. These vessels travel along the surface of the femoral neck before entering the head. Intracapsular fractures can interrupt this pathway, reducing or completely stopping perfusion to the femoral head.
When blood supply is inadequate, osteocytes, the cells responsible for maintaining bone tissue, undergo ischaemic necrosis. This process develops over time rather than immediately and may not be evident on early imaging. As dead bone loses structural strength, the femoral head may collapse months after the initial injury, leading to pain, joint dysfunction and failure of fixation. This delayed but predictable risk explains why joint replacement is often preferred over internal fixation for many intracapsular neck of femur fractures.
Biomechanics and fracture pattern
The femoral neck is exposed to substantial bending and shear forces during normal weight-bearing. In healthy bone, the trabecular network within the femoral neck distributes these forces efficiently. In osteoporotic bone, trabeculae become thinner and less interconnected, reducing the bone’s ability to absorb load and making it more susceptible to fracture under relatively minor stress.
Once the femoral neck is fractured, continuity between the femoral head and shaft is lost. Muscle forces acting on the femur, particularly from the iliopsoas and external rotators, pull the limb into external rotation and cause apparent shortening. These physical signs arise from mechanical displacement of bone fragments rather than from direct muscle injury and are important clinical indicators of fracture.
Immobility and systemic consequences
Neck of femur fractures result in immediate loss of independent mobility. Even short periods of immobility lead to rapid physiological change, including reduced lung expansion, venous stasis in the lower limbs and slowed gastrointestinal motility. Older adults are especially vulnerable because age-related reductions in cardiovascular, respiratory and neuromuscular reserve limit their ability to compensate.
Fracture also triggers a systemic inflammatory response and activation of stress hormones, increasing metabolic demand at a time when oral intake and activity are reduced. This imbalance contributes to delirium, infection, thromboembolism and pressure injury. These complications arise not from the fracture alone, but from the interaction between injury, immobility and reduced physiological resilience.
Surgical timing and physiological stress
Early surgical intervention is prioritised to stabilise the fracture and limit the duration of immobility and systemic stress. Delayed surgery prolongs the inflammatory and catabolic state, increases pain burden and heightens the risk of secondary complications such as pneumonia, delirium and venous thromboembolism.
The choice of surgical approach depends on both fracture location and biological risk. Intracapsular fractures are frequently managed with hemiarthroplasty or total hip replacement to avoid complications related to impaired blood supply and poor healing. Extracapsular fractures are more commonly treated with internal fixation, allowing bone healing to occur while restoring mechanical stability. These decisions are driven by fracture biology and biomechanics rather than by patient age alone.
Clinical Connections
Neck of femur fractures commonly present with groin or hip pain, inability to weight-bear, limb shortening and external rotation of the affected leg. Pain may be minimal at rest, particularly in older adults with cognitive impairment, neurological disease or communication barriers, which can delay recognition and imaging. Because these fractures disrupt load transmission across the hip, attempts to stand or transfer often provoke sudden pain or collapse rather than gradual limitation. Diagnosis is confirmed with pelvic or hip radiography, with further imaging such as CT or MRI used when clinical suspicion remains high despite normal initial films.
Several early features guide clinical assessment and escalation:
Inability to weight-bear following a fall, even when pain appears mild
Limb shortening and external rotation caused by loss of femoral neck continuity
Disproportionate functional decline compared with visible injury
Complications following neck of femur fracture are most often systemic rather than local to the hip. Acute pain, blood loss and inflammatory activation trigger a physiological stress response, while immobility rapidly leads to deconditioning. Reduced lung expansion increases pneumonia risk, venous stasis promotes thromboembolism, and altered hydration, pain and unfamiliar environments contribute to delirium. These processes develop quickly, particularly in older adults with limited physiological reserve.
Management priorities target both the fracture and its whole-body consequences. Early surgery limits ongoing pain, inflammatory burden and immobility, while timely mobilisation reduces respiratory, thrombotic and pressure-related complications. Adequate analgesia supports participation in movement and reduces stress responses, and multidisciplinary care addresses hydration, nutrition, cognition and functional recovery. Outcomes following neck of femur fracture are therefore shaped less by the fracture pattern alone and more by how rapidly the systemic effects of injury and immobility are interrupted.
Concept Check
Why does fracture location within or outside the joint capsule affect healing potential?
How does disruption of femoral head blood supply lead to avascular necrosis?
Why are NOF fractures strongly associated with osteoporosis?
How does immobility following NOF fracture contribute to systemic complications?
Why is early surgical intervention prioritised in NOF fracture management?