Proprioception & Stretch Reflexes
Proprioception is the body’s ability to sense position, movement, and force without visual input. It allows humans to walk without watching their feet, grasp objects without looking, and maintain posture without conscious effort. This sensory system depends on specialised mechanoreceptors embedded within muscles and tendons that continuously relay information to the central nervous system. Two structures play the dominant role in this system: muscle spindles, which monitor muscle length, and Golgi tendon organs, which monitor muscle tension. Together, they form the foundation of reflex control, coordination, balance, and injury prevention.
What You Need to Know
Proprioception is the nervous system’s internal sense of body position, movement, and force. It allows the brain to know where each limb is, how fast it’s moving, and how much tension is being produced, even without visual input. This information is essential for balance, posture, coordination, and safe movement, because the brain relies on continuous feedback from the body to guide motor control and prevent injury.
Proprioception is maintained through specialised sensory receptors that continuously monitor muscle activity and position, including:
Muscle spindles detect muscle length and the speed of stretch
Golgi tendon organs detect muscle tension and force
Both send continuous sensory information to the spinal cord, cerebellum, and cerebral cortex. This crease a real-time map of body position and movement.
Proprioceptive signals are used in two main ways. Some are processed at the spinal cord level to generate rapid, automatic reflexes that stabilise joints and protect muscles from excessive stretch or overload. Others travel to the cerebellum and cerebral cortex, where they contribute to conscious awareness of limb position and allow movements to be refined and coordinated with vision and balance.
Muscle spindles and Golgi tendon organs form the sensory foundation of motor control. By constantly monitoring muscle length and tension, they ensure that contractions are appropriately timed and scaled to the task being performed. This continuous feedback allows movements to remain smooth, efficient, and precisely controlled, whether standing still, walking, or performing fine motor tasks.
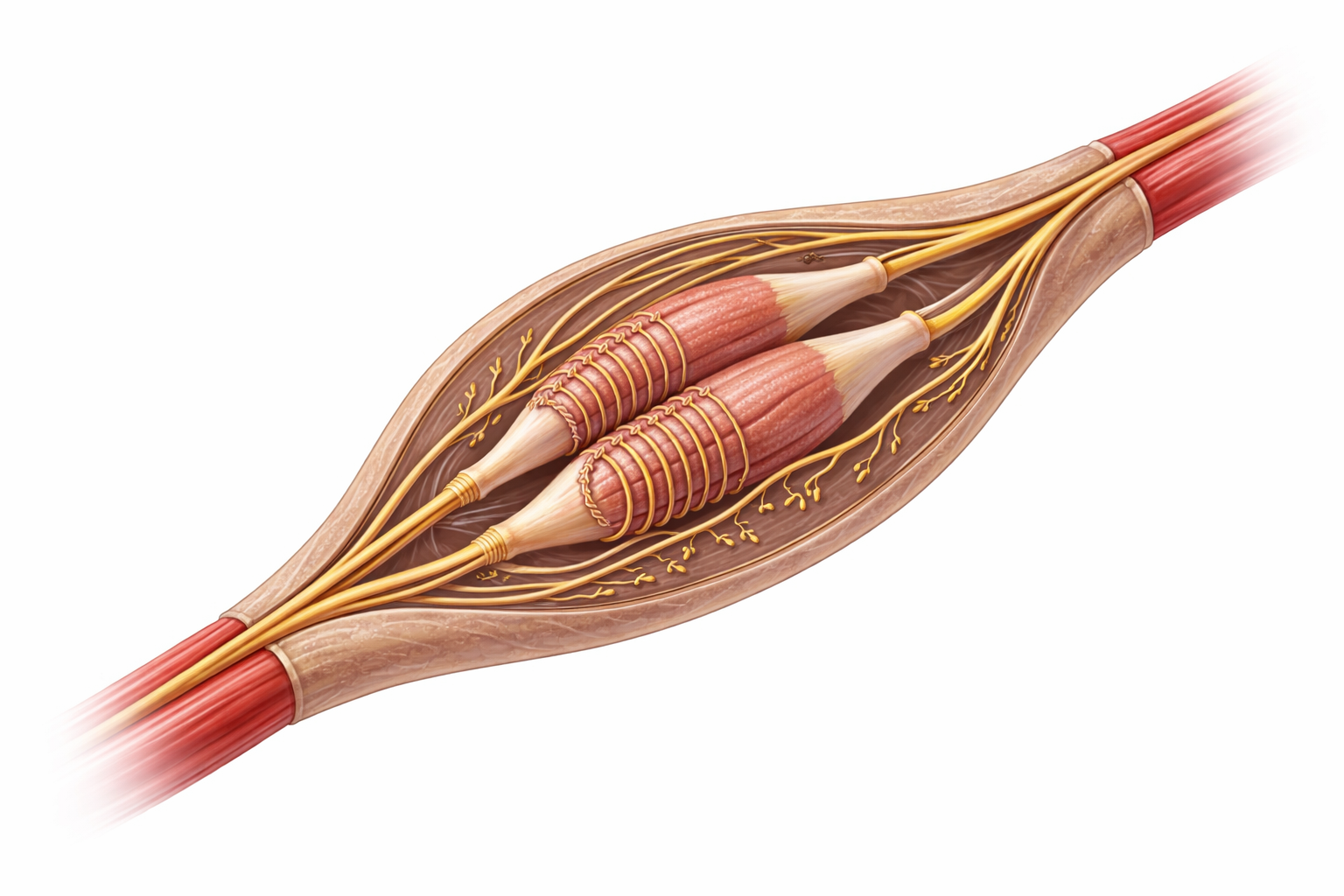
Image: Muscle spindle within skeletal muscle, showing intrafusal fibres enclosed in a connective tissue capsule, with sensory endings wrapped around the central region and motor endings at the poles, enabling detection of muscle stretch and adjustment of muscle tone.
Beyond the Basics
Muscle Spindles and the Stretch Reflex
Muscle spindles are small, spindle-shaped sensory organs located parallel to skeletal muscle fibres. They contain specialised intrafusal fibres (modified muscle fibres designed for sensing rather than force production) that detect changes in muscle length and the rate at which a muscle is being stretched. When a muscle lengthens, the muscle spindle is deformed, activating sensory endings that send rapid afferent signals (signals travelling toward the spinal cord) through sensory neurons.
This input triggers the stretch reflex, also known as the myotatic reflex. The sensory neuron synapses directly with the alpha motor neuron supplying the same muscle, producing an immediate contraction in response to stretch. At the same time, inhibitory interneurons suppress the antagonist muscle, a process called reciprocal inhibition, allowing smooth and efficient movement. This reflex stabilises joints, maintains posture, and prevents excessive muscle lengthening that could damage fibres.
The stretch reflex operates continuously during standing and movement, automatically adjusting muscle tone to compensate for shifts in body position, gravity, and load. It is also the physiological basis of clinical tendon reflex testing, where tapping a tendon briefly stretches the muscle and triggers a visible contraction.
Gamma Motor Neurons and Sensitivity Control
Muscle spindle sensitivity is regulated by gamma motor neurons, which innervate the contractile ends of intrafusal fibres. When gamma motor activity increases, the intrafusal fibres shorten slightly, keeping the spindle taut and more responsive to stretch. This increases the sensitivity of the spindle, enhancing postural tone and reflex responsiveness.
During voluntary movement, alpha and gamma motor neurons are activated together, a process known as alpha–gamma coactivation. This ensures that muscle spindles continue to provide accurate length feedback even as the muscle shortens, preventing the sensory system from becoming “slack” and losing sensitivity during contraction.
Golgi Tendon Organs and Tension Regulation
Golgi tendon organs (GTOs) are located at the junction between muscle fibres and their tendons. Unlike muscle spindles, which detect muscle length, GTOs monitor muscle tension, particularly during active contraction. When tension becomes excessive, GTOs activate inhibitory interneurons in the spinal cord that reduce alpha motor neuron activity to that muscle.
This produces autogenic inhibition, a protective reflex that causes the muscle to relax before structural damage occurs. It acts as a built-in safety mechanism that limits excessive force and prevents tendon or muscle rupture. With training, the nervous system can adjust GTO sensitivity, allowing greater force generation before inhibitory signals are triggered, which is one reason strength improves with conditioning.
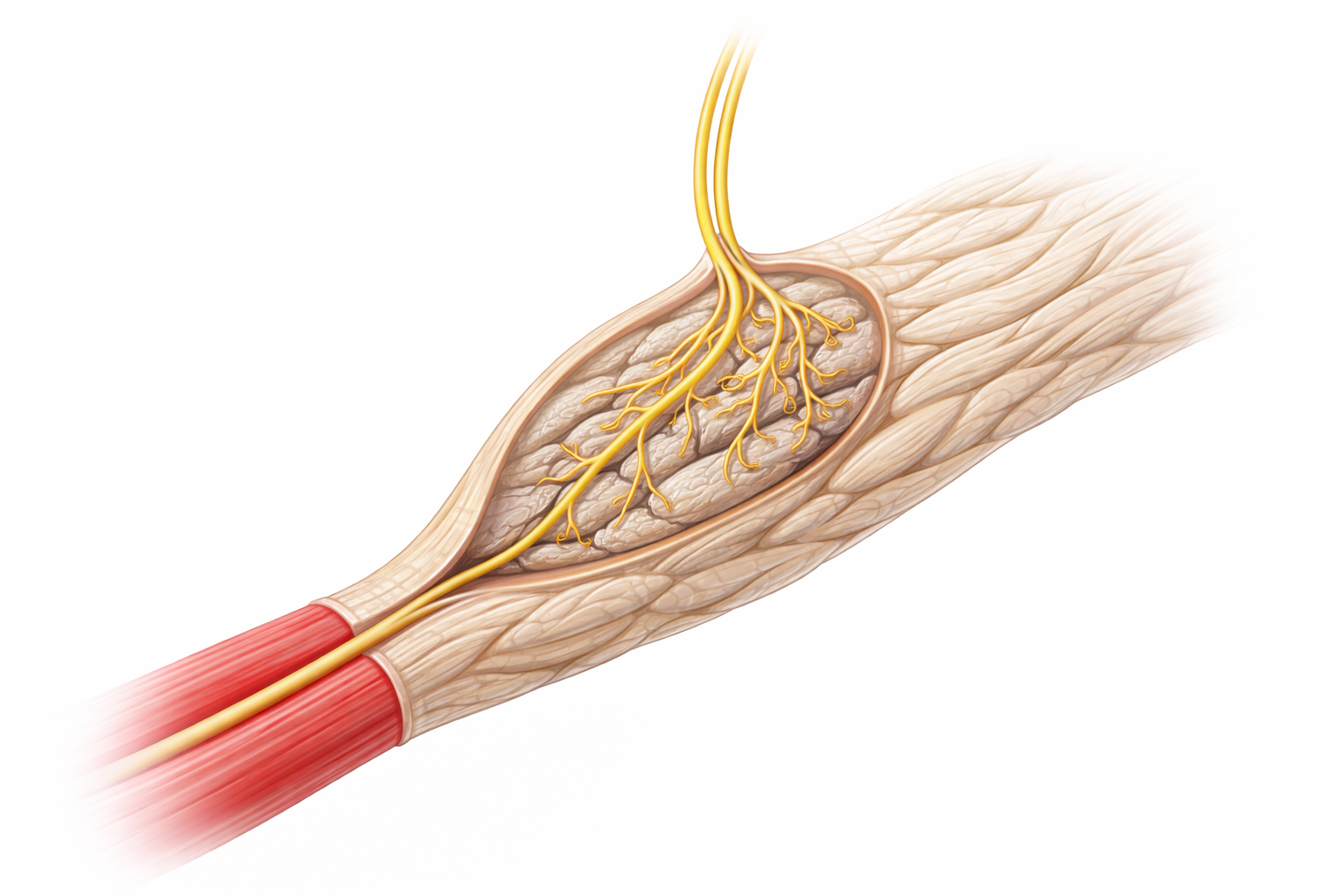
Image: Golgi tendon organ located at the muscle–tendon junction, showing collagen fibres within a connective tissue capsule with a single sensory nerve fibre branching between them to detect muscle tension and force.
Proprioception in Coordinated Movement
Information from muscle spindles and Golgi tendon organs is integrated with input from joint receptors, the vestibular system (balance organs of the inner ear), and vision. This integration occurs at multiple levels of the nervous system, including the spinal cord, cerebellum, and cerebral cortex, allowing the brain to continuously update its internal map of body position and movement.
Proprioceptive feedback is essential for fine motor control, joint stability, and balance. When this system is impaired, as in peripheral neuropathy or spinal cord disease, movements become clumsy, poorly timed, and unsafe, even when muscle strength is preserved. Coordinated movement depends not only on strong muscles, but on accurate and continuous sensory feedback.
Clinical Connections
Damage to proprioceptive pathways produces profound movement dysfunction because the brain no longer receives accurate information about limb position, joint stability, and muscle tension. In peripheral neuropathy, sensory fibres from muscle spindles and joint receptors are damaged, so patients lose reliable feedback from their feet and legs. This leads to a wide-based, unsteady gait, difficulty judging foot placement, and a high risk of falls, particularly in low-light conditions when vision cannot compensate.
In cerebellar disorders, proprioceptive signals still reach the brain, but they cannot be integrated properly. The cerebellum fails to compare intended movement with actual movement, producing ataxia, tremor, overshooting of targets (dysmetria), and poor coordination. These patients often appear weak, but the primary problem is faulty timing and error correction rather than muscle strength.
Disruption of proprioceptive pathways leads to characteristic functional deficits depending on the site of injury, including:
Peripheral sensory loss: unsteady gait, poor joint awareness, falls
Cerebellar dysfunction: ataxia, dysmetria, tremor, poor coordination
Joint injury: impaired proprioceptive input and chronic instability
Spinal or cortical lesions: abnormal reflexes and muscle tone
After joint injuries such as ankle sprains, ACL tears, or ligament ruptures, proprioceptive receptors in the joint capsule and surrounding tissues are damaged. Even when the joint heals structurally, the nervous system may no longer receive accurate position and tension information. This leads to chronic instability, poor balance, and a high risk of re-injury unless targeted rehabilitation restores neuromuscular control. Balance training, wobble boards, and functional movement exercises work by retraining proprioceptive pathways and improving reflex stability.
In spinal cord injury and stroke, disruption of descending motor control alters how reflex circuits behave. Loss of inhibitory input from the brain causes stretch reflexes to become exaggerated, producing spasticity, clonus, and rigidity. In contrast, damage to lower motor neurons or sensory afferents abolishes reflexes and leads to flaccid weakness and muscle wasting. These changes affect mobility, posture, and safety, and they guide clinical assessment, prognosis, and rehabilitation planning.
Concept Check
Why does the stretch reflex help maintain posture during standing?
How do gamma motor neurons adjust muscle spindle sensitivity?
Why do Golgi tendon organs inhibit excessive force production?
Why does proprioceptive loss increase fall risk even if muscle strength is normal?
Why is balance training essential after joint injury?