Micturition Physiology: Neural Control of Bladder Filling and Emptying
Micturition, the process of storing and voiding urine, is a coordinated interaction between the urinary bladder, urethral sphincters, and the nervous system. Although the kidneys are responsible for producing urine, the lower urinary tract controls when and how urine is eliminated. This system operates through a balance of autonomic and somatic pathways that shift between storage mode and voiding mode according to the body’s needs. Understanding these mechanisms is essential for recognising why urinary dysfunction occurs in neurological injury, spinal cord lesions, postoperative patients, and age-related changes.
What You Need to Know
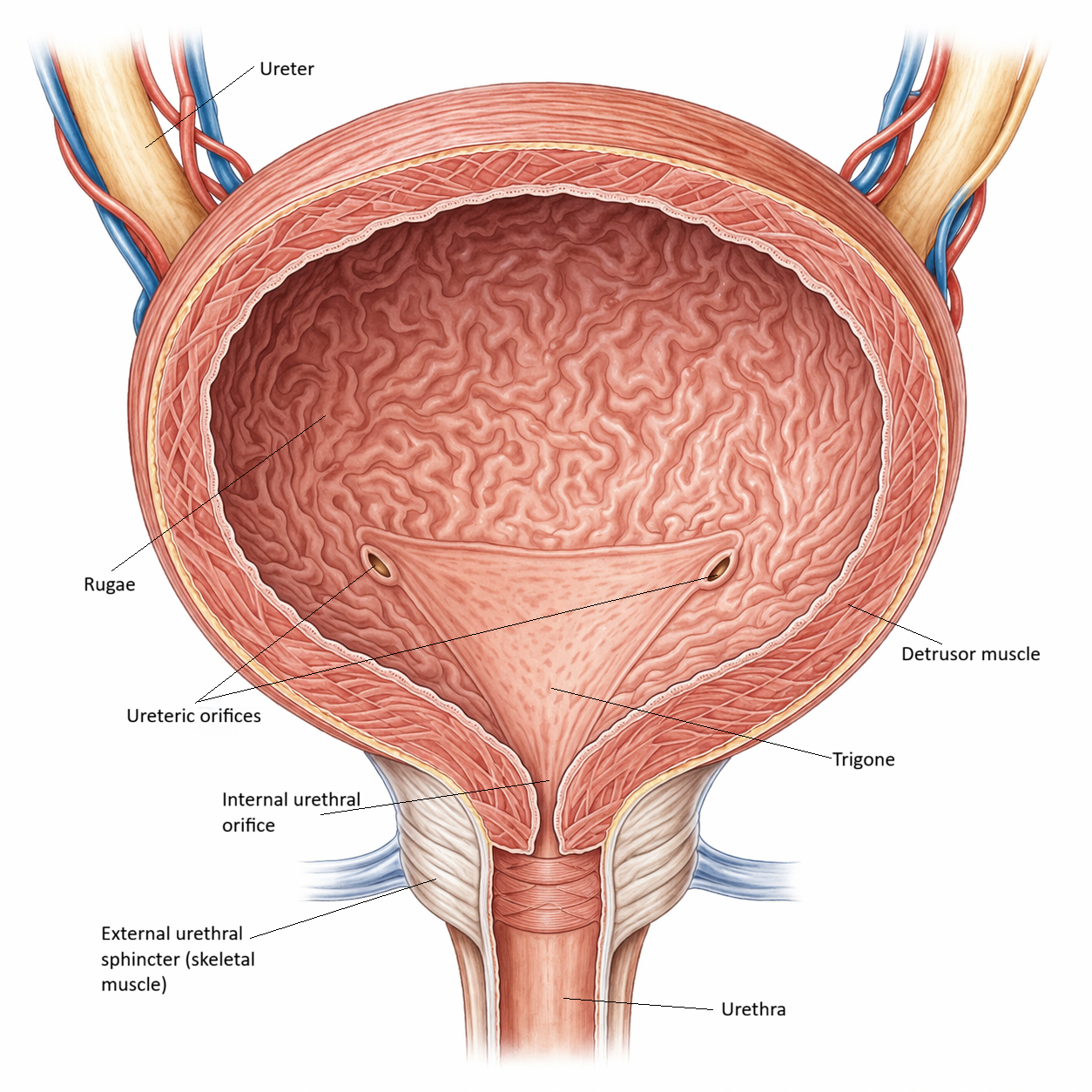
Micturition is a highly regulated process that alternates between two functional phases: bladder storage and bladder emptying. These phases depend on coordinated activity between the detrusor muscle, the internal urethral sphincter, and the external urethral sphincter, which function together as a single integrated unit. Rather than being a simple reflex, micturition balances involuntary autonomic control with conscious voluntary input, allowing urine to be stored safely for prolonged periods and expelled efficiently at an appropriate time.
During the storage phase, the bladder fills at low pressure. The detrusor muscle remains relaxed while both urethral sphincters stay contracted, enabling increasing volumes of urine to be accommodated without leakage. Stretch receptors within the bladder wall continuously sense filling and transmit afferent signals to the spinal cord and brainstem. These signals create awareness of bladder volume but are actively suppressed from triggering voiding by higher brain centres.
This storage state is maintained through coordinated neural pathways:
sympathetic nerves, which inhibit detrusor contraction and tighten the internal urethral sphincter
parasympathetic nerves, which remain relatively inactive during filling
somatic motor nerves, which maintain voluntary contraction of the external urethral sphincter
As bladder volume increases, afferent signalling intensifies and activates the micturition reflex at the spinal level. Voiding, however, only occurs when higher cortical centres permit it. When micturition is initiated, parasympathetic activity increases, causing the detrusor muscle to contract while the internal urethral sphincter relaxes. Voluntary relaxation of the external urethral sphincter removes the final outflow resistance. This coordinated switch from storage to emptying allows controlled, complete bladder evacuation while maintaining continence at all other times.
Beyond the Basics
Bladder structure and receptive relaxation
As urine enters the bladder, the detrusor muscle accommodates increasing volume with minimal rise in intravesical pressure, a property known as receptive relaxation. This is essential for effective urine storage and is enabled by the elastic connective tissue of the bladder wall, the intrinsic properties of smooth muscle, and continuous modulation by sympathetic neural input. Stretch receptors embedded within the bladder wall monitor filling and transmit afferent signals centrally.
As bladder volume approaches functional capacity (he maximum volume of urine a bladder can comfortably hold while functioning normally), typically around 350–500 mL in adults, stretch receptor firing increases. This rising afferent activity generates a conscious awareness of bladder fullness and signals that voiding may soon be required, without automatically triggering emptying.
Sympathetic control and the storage phase
During the storage phase, sympathetic nervous system activity predominates via the hypogastric nerve. Sympathetic fibres promote relaxation of the detrusor muscle and contraction of the internal urethral sphincter, allowing the bladder to fill while maintaining continence. Detrusor relaxation is mediated primarily through β₃-adrenergic receptors, while α₁-adrenergic receptors increase smooth muscle tone at the bladder neck. This coordinated sympathetic influence maintains bladder compliance and keeps the outflow tract closed, enabling urine storage during normal activities such as standing, walking, or coughing without leakage.
Somatic control and voluntary sphincter regulation
The external urethral sphincter is innervated by the pudendal nerve and is under voluntary somatic control. During bladder filling, this sphincter remains tonically contracted, providing conscious suppression of voiding even as afferent signals from stretch receptors increase.
Voluntary control over the external sphincter allows individuals to delay micturition until socially appropriate. The ability to consciously contract and relax this sphincter represents a critical developmental milestone in continence and remains central to adult bladder control.
Although voluntary control over the external urethral sphincter allows conscious delay of micturition, this control is not unlimited. As bladder volume increases, afferent signalling intensifies and reflex pathways become progressively more dominant, increasing detrusor contractility and the sensation of urgency. Beyond a certain threshold, sustained sphincter contraction becomes difficult to maintain, and voiding may occur involuntarily if the pressure generated by the detrusor overcomes sphincter resistance.
Parasympathetic control and the voiding phase
When voiding is initiated, neural control shifts toward parasympathetic dominance via the pelvic nerves. Parasympathetic fibres release acetylcholine, stimulating muscarinic receptors on detrusor smooth muscle and producing a strong, coordinated contraction. At the same time, sympathetic tone is withdrawn and both the internal and external urethral sphincters relax.
This coordinated pattern allows bladder pressure to rise sufficiently to overcome urethral resistance, producing a smooth and continuous urine stream. The switch from storage to voiding is orchestrated by the pontine micturition centre, which synchronises detrusor contraction with sphincter relaxation.
Neural integration and higher brain control
Although the micturition reflex is present at birth, voluntary control emerges as higher brain centres mature. In adults, the prefrontal cortex, hypothalamus, and pontine micturition centre work together to integrate sensory input, emotional context, and social appropriateness.
When voiding is inappropriate, cortical centres inhibit the pontine micturition centre and reinforce storage by maintaining external sphincter contraction. When voiding is permitted, cortical inhibition is withdrawn, allowing the reflex to proceed. Disruption of these pathways, as seen in conditions such as spinal cord injury, multiple sclerosis, stroke, or Parkinson’s disease, produces predictable patterns of urgency, retention, incontinence, or detrusor–sphincter dyssynergia.
Pressure dynamics and bladder compliance
A healthy bladder maintains low internal pressure throughout most of the filling phase, protecting the upper urinary tract from pressure transmission. As long as the detrusor remains relaxed and sphincter closure is maintained, bladder pressure rises only minimally despite increasing volume.
During voiding, coordinated detrusor contraction raises intravesical pressure enough to expel urine effectively. Loss of bladder compliance, as occurs with chronic outlet obstruction, inflammation, or fibrosis, results in elevated filling pressures. Sustained pressure elevation can transmit backward toward the ureters and renal pelvis, increasing the risk of vesicoureteral reflux, hydronephrosis, and progressive kidney damage.
Clinical Connections
The physiology of micturition provides a clear framework for understanding many common disorders of bladder storage and emptying. Because continence and voiding depend on precise coordination between detrusor contraction, sphincter relaxation, and neural control, disruption at any point in this system produces characteristic and predictable clinical patterns.
Urinary Retention
Urinary retention most often results from failure of effective bladder emptying. This may occur due to impaired detrusor contraction, as seen in diabetic autonomic neuropathy or acute postoperative states, excessive outlet resistance from increased sphincter tone, or mechanical obstruction such as benign prostatic hyperplasia. In these situations, bladder pressure fails to rise adequately or outflow resistance remains too high, leading to incomplete emptying and progressive bladder distension.
Urinary retention can occur when normal bladder emptying is disrupted by neurological, pharmacological, anatomical, or functional factors. Common causes include:
Post-operative urinary retention – Anaesthesia, pain, immobility, and temporary disruption of bladder reflexes can impair normal voiding
Opioid medications – Reduce detrusor muscle contraction and increase urethral sphincter tone, making bladder emptying more difficult
Anticholinergic medications – Inhibit parasympathetic stimulation of the bladder, reducing detrusor muscle activity
Benign prostatic hyperplasia (BPH) – Enlargement of the prostate obstructs urine flow through the urethra
Neurological disorders – Conditions such as spinal cord injury, multiple sclerosis, Parkinson's disease, and diabetic neuropathy may disrupt neural control of micturition
Severe constipation or faecal impaction – Rectal distension can compress the bladder neck or interfere with normal bladder function
Urethral obstruction – Urethral strictures, urinary calculi, blood clots, or tumours may physically block urine flow
Pain or discomfort – Perineal pain, surgical wounds, or fear of movement may cause patients to suppress the urge to void
Pelvic organ prolapse – Altered pelvic anatomy may impair bladder emptying in some individuals
Urinary tract infection – Inflammation and swelling may contribute to temporary urinary retention, particularly in older adults
Overdistension of the bladder – Prolonged delays in voiding can overstretch the detrusor muscle and impair its ability to contract effectively
Psychological factors – Anxiety, unfamiliar environments, or lack of privacy may inhibit normal voiding despite adequate bladder filling
Postoperative urinary retention is a commonly identified and escalated by nursing staff. It is usually a transient manifestation of disrupted micturition physiology. A combination of anaesthesia, pain, opioid use, and immobility reduce parasympathetic activity and detrusor contractility while increasing outlet resistance, delaying the normal switch from storage to voiding. Postoperative urinary retention may be treated with temporary catheterisation, followed by a trial of voiding without a urinary catheter (trial of void).
Urinary Incontinence
In contrast, urge incontinence typically results from detrusor overactivity. Here, involuntary detrusor contractions occur during the storage phase, overcoming sphincter resistance and producing urgency, frequency, and leakage. This pattern is common in ageing, neurological disease, and conditions affecting sensory signalling from the bladder wall.
Depending on the underlying cause, incontinence may result from increased bladder pressure, impaired sphincter function, involuntary bladder contractions, neurological dysfunction, or an inability to reach the toilet in time. Common causes include:
Stress incontinence – Weakness of the pelvic floor muscles or urethral sphincter allows urine leakage during activities that increase intra-abdominal pressure, such as coughing, sneezing, or lifting
Urge incontinence – Involuntary detrusor muscle contractions create a sudden, intense urge to void that may be difficult to suppress
Overactive bladder – Increased bladder sensitivity and detrusor overactivity result in urinary urgency, frequency, and sometimes urge incontinence
Pelvic floor dysfunction – Damage or weakening of the pelvic floor, often associated with pregnancy, childbirth, ageing, or menopause, reduces support for the bladder and urethra
Neurological disorders – Conditions such as stroke, multiple sclerosis, Parkinson's disease, spinal cord injury, and dementia may disrupt neural control of continence
Urinary tract infection – Bladder irritation and inflammation can increase urgency and contribute to temporary episodes of incontinence
Benign prostatic hyperplasia (BPH) – Prostatic enlargement may impair bladder emptying and contribute to overflow incontinence
Overflow incontinence – Chronic urinary retention causes the bladder to become overdistended, resulting in frequent leakage of small amounts of urine
Functional incontinence – Physical, cognitive, or environmental barriers prevent an individual from reaching the toilet despite normal urinary function
Medications – Diuretics, sedatives, alpha-blockers, and some antidepressants may contribute to urinary leakage through various mechanisms
Chronic cough or obesity – Repeated increases in intra-abdominal pressure can place strain on pelvic floor structures and worsen stress incontinence
Cognitive impairment – Conditions such as dementia may affect the ability to recognise the need to void or locate and use toileting facilities appropriately
Management should focus on maintaining dignity, comfort, hygiene, and skin integrity. Strategies may include scheduled toileting, pelvic floor exercises, continence aids, medication, or treatment of the underlying cause. Ongoing exposure to urine can cause skin maceration, irritation, and incontinence-associated dermatitis, increasing susceptibility to skin breakdown. Excess moisture also reduces the skin's tolerance to pressure and shear forces, increasing the risk of pressure injuries, particularly in vulnerable areas such as the sacrum, buttocks, and perineum. Regular skin assessment, prompt cleansing after episodes of incontinence, and the use of appropriate barrier products are therefore important aspects of nursing care.
Concept Check
How does the sympathetic nervous system support the bladder’s storage function?
Why is the pontine micturition centre essential for coordinated voiding?
What roles do the internal and external urethral sphincters play during each phase of micturition?
How would a spinal cord injury above the sacral segments affect bladder function?
Why does loss of bladder compliance threaten kidney health?