Ureters and Urethra: Structure, Histology and Functional Organisation
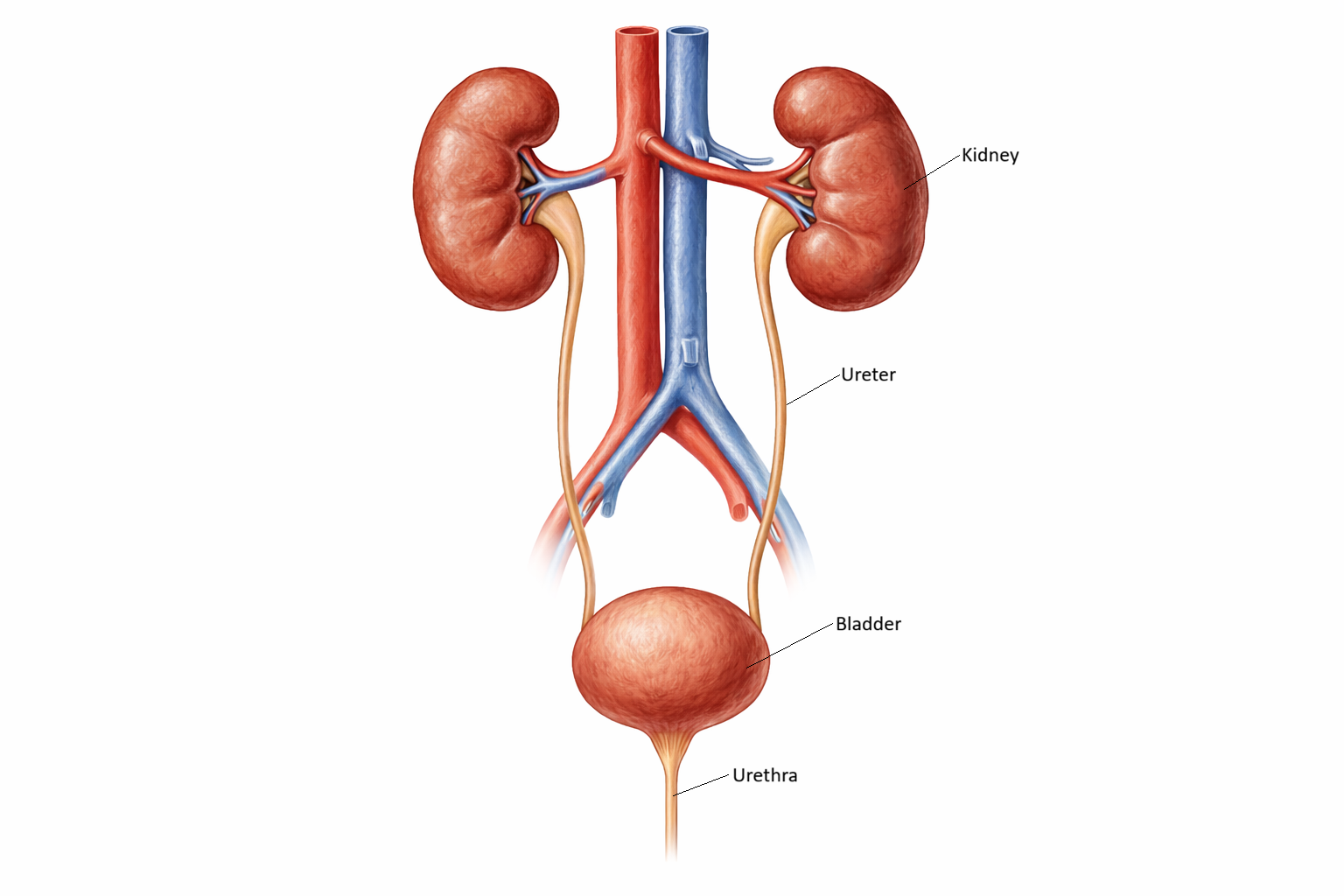
The ureters and urethra form the conduits that transport urine from the kidneys to the external environment. Although they appear simple compared with the kidneys and bladder, their structure is intricately adapted to ensure the safe, one-way movement of urine while preventing reflux, obstruction and infection. The ureters use coordinated muscular contractions to propel urine toward the bladder, while the urethra provides the final passage for urine expulsion and contributes to continence. Their anatomy underpins essential clinical concepts such as kidney stone obstruction, urinary reflux, pelvic floor dysfunction and catheterisation safety.
What You Need to Know
The ureters and urethra form the lower urinary tract pathways responsible for transporting urine, preventing reflux, and enabling controlled storage and elimination. The ureters are narrow, muscular tubes that convey urine from the renal pelvis to the bladder through coordinated peristaltic contractions. Their wall structure is specifically adapted for this function, combining a distensible epithelial lining with a strong muscular layer that can propel urine independently of gravity.
A key protective feature of the ureters is their oblique entry into the bladder wall. As the bladder fills and pressure rises, this angled passage is compressed, forming a functional one-way valve that prevents backflow of urine toward the kidneys. This arrangement is essential for protecting renal tissue from pressure-related injury and ascending infection.
The urethra shows greater anatomical variation, particularly between sexes, reflecting differences in length, surrounding structures, and functional demands. Despite these differences, several shared structural and functional principles apply:
a mucosal lining adapted to urine exposure and, in distal regions, friction during voiding
smooth and skeletal muscle layers that contribute to continence and coordinated emptying
sphincter mechanisms, including involuntary smooth muscle control and voluntary skeletal muscle control
Together, the ureters and urethra integrate structural specialisation with neural and muscular control to ensure unidirectional urine flow, protection of the upper urinary tract, and precise regulation of voiding. Their coordinated function is essential for maintaining urinary continence and preserving renal health.
Beyond the Basics
Ureters
The ureters extend from the renal pelvis to the posterior aspect of the bladder, descending retroperitoneally along the psoas muscle before curving medially into the pelvis. As each ureter enters the bladder wall, it passes obliquely through the detrusor muscle and mucosa to form the ureterovesical junction. This angled entry acts as a functional one-way valve, which is compressed as bladder pressure rises during filling or micturition, preventing reflux of urine toward the kidneys.
The ureteral wall is composed of several specialised layers that support both distension and active propulsion. The mucosa is lined with transitional epithelium, allowing repeated stretching and recoil without structural damage. Beneath this lies the lamina propria, a connective tissue layer rich in elastic fibres and small blood vessels that support epithelial integrity. The muscularis forms the bulk of the ureter and generates peristaltic activity. In the upper two-thirds, it consists of an inner longitudinal and outer circular layer, while an additional outer longitudinal layer appears in the distal third, strengthening propulsion as urine approaches the bladder.
Surrounding the muscularis is an adventitial layer that anchors the ureter within the retroperitoneum and carries its blood vessels, lymphatics, and nerves. Although sympathetic and parasympathetic fibres modulate peristaltic frequency, ureteral smooth muscle possesses intrinsic pacemaker activity, allowing urine transport to continue even when neural input is reduced.
The ureters have three anatomical narrowing points: the ureteropelvic junction, the point where the ureter crosses the pelvic brim, and the ureterovesical junction. These sites are particularly important because urinary calculi commonly lodge there, producing predictable patterns of colicky pain and obstruction.
Urethra
The urethra conducts urine from the bladder to the exterior and plays a central role in continence through coordinated sphincter control. While both sexes share similar histological layers, including mucosa, connective tissue, and muscle, the length, segmentation, and surrounding anatomy differ substantially between females and males.
In females, the urethra is short and relatively straight, measuring approximately four centimetres. The mucosal lining transitions from transitional epithelium proximally to stratified squamous epithelium distally, reflecting increasing exposure to friction. The underlying connective tissue contains abundant elastic fibres and a venous plexus that contributes to urethral closure by engorging during continence. A smooth muscle internal sphincter is present at the bladder neck, while the external urethral sphincter, composed of skeletal muscle under somatic control, surrounds the mid-urethra and integrates with the pelvic floor musculature.
This anatomical arrangement supports voluntary continence but also increases susceptibility to urinary tract infection, as the short urethral length provides a shorter pathway for ascending bacteria.
In males, the urethra is considerably longer, measuring approximately 18 to 20 centimetres, and is divided into three segments. The prostatic urethra passes through the prostate gland and receives the ejaculatory ducts, serving both urinary and reproductive functions. The membranous urethra is the narrowest segment and traverses the urogenital diaphragm, where it is surrounded by the external urethral sphincter. The spongy urethra runs within the corpus spongiosum of the penis and opens at the external urethral meatus.
Epithelial lining varies along the male urethra, transitioning from transitional epithelium proximally to pseudostratified columnar and then stratified squamous epithelium distally. This variation reflects differences in mechanical stress and functional role. The length and curvature of the male urethra increase resistance to infection but also make catheterisation more technically complex and raise the risk of urethral trauma.
Sphincters and continence mechanisms
Urinary continence depends on the coordinated function of two sphincter systems. The internal urethral sphincter consists of smooth muscle fibres at the bladder neck and provides involuntary closure during bladder filling. This mechanism is particularly well developed in males, where it also prevents retrograde ejaculation.
The external urethral sphincter is composed of skeletal muscle innervated by the pudendal nerve, allowing voluntary control over micturition. Its integration with pelvic floor musculature provides additional support during increases in intra-abdominal pressure.
Continence reflects the balance between urethral closure pressure and bladder pressure. Disruption of sphincter integrity, pelvic floor support, neural pathways, or urethral structure compromises this balance and may result in urinary incontinence or retention, particularly in the context of ageing, childbirth, neurological disease, or pelvic surgery.
Clinical Connections
The structural organisation of the ureters directly explains the characteristic patterns of pain, obstruction, and functional preservation seen in clinical practice. Narrowing points along the ureter create predictable sites where kidney stones, strictures, or external compression are most likely to impede urine flow, producing colicky flank pain that may radiate as peristaltic waves intensify against an obstruction. Importantly, ureteric smooth muscle possesses intrinsic pacemaker activity, which allows peristalsis to continue even in the absence of autonomic innervation. This explains why transplanted kidneys are able to drain urine effectively despite loss of normal neural connections.
Anatomical differences within the urethra underpin sex-specific patterns of disease and procedural risk. The short, relatively straight female urethra increases susceptibility to ascending urinary tract infection, while reliance on pelvic floor support makes continence vulnerable to childbirth, ageing, and pelvic surgery. In males, the length and segmentation of the urethra introduce distinct sites of obstruction and injury, particularly in the presence of prostate enlargement or urethral narrowing.
Common clinical conditions that reflect ureteric and urethral structure include:
renal colic and obstructive uropathy, resulting from calculi lodging at physiological narrowing points
benign prostatic hyperplasia, causing bladder outlet obstruction at the prostatic urethra
urethral strictures, which disrupt laminar urine flow and increase infection and retention risk
stress and urge incontinence, related to sphincter integrity and pelvic floor support
Understanding lower urinary tract anatomy is also essential for safe clinical practice. Knowledge of urethral length, curvature, and sphincter location informs appropriate catheter selection and insertion technique, reducing the risk of false passage, urethral trauma, and infection.
Concept Check
Why do the ureters enter the bladder at an oblique angle and how does this protect the kidneys
How does the muscular arrangement of the ureter support peristaltic urine transport
Why are kidney stones more likely to lodge at the ureteropelvic junction, pelvic brim and ureterovesical junction
How do structural differences between the male and female urethra influence infection risk and continence
Why is the external urethral sphincter essential for voluntary control of urination