Cervical Cancer: HPV-Driven Dysplasia, Malignant Transformation, and Local Invasion
Cervical cancer is a malignancy arising from the cervical epithelium, most commonly driven by persistent infection with high-risk human papillomavirus (HPV). Unlike many cancers, cervical cancer develops through a well-defined, stepwise progression from normal epithelium to dysplasia and invasive disease. Cervical cancer may remain asymptomatic for years, which is why screening is highly effective. Advanced disease often presents with bleeding, pain, and local organ involvement.
What You Need to Know
The cervix is lined by two distinct epithelial types that meet at the transformation zone, where glandular columnar epithelium of the endocervix transitions to stratified squamous epithelium of the ectocervix. This region undergoes continuous remodelling, with cells regularly being replaced and exposed to the vaginal environment. The combination of active cell turnover and exposure to potential pathogens makes the transformation zone particularly susceptible to infection, especially by oncogenic strains of human papillomavirus (HPV).
Key features of cervical cancer development include:
persistent infection with high-risk HPV types, most commonly HPV 16 and 18
viral entry into basal epithelial cells through microabrasions
integration of viral DNA into host cell genomes
disruption of tumour suppressor proteins such as p53 and Rb
progressive changes from dysplasia to invasive carcinoma over time
Cervical cancer develops when high-risk HPV infection is not cleared by the immune system and instead persists within epithelial cells. Viral proteins interfere with normal cell-cycle regulation, allowing uncontrolled proliferation and accumulation of genetic damage. Over time, this leads to a spectrum of precancerous changes, from low-grade dysplasia to high-grade lesions, before progressing to invasive cancer. This process is driven primarily by viral-mediated disruption of tumour suppressor pathways, rather than by hormonal or inflammatory mechanisms alone.
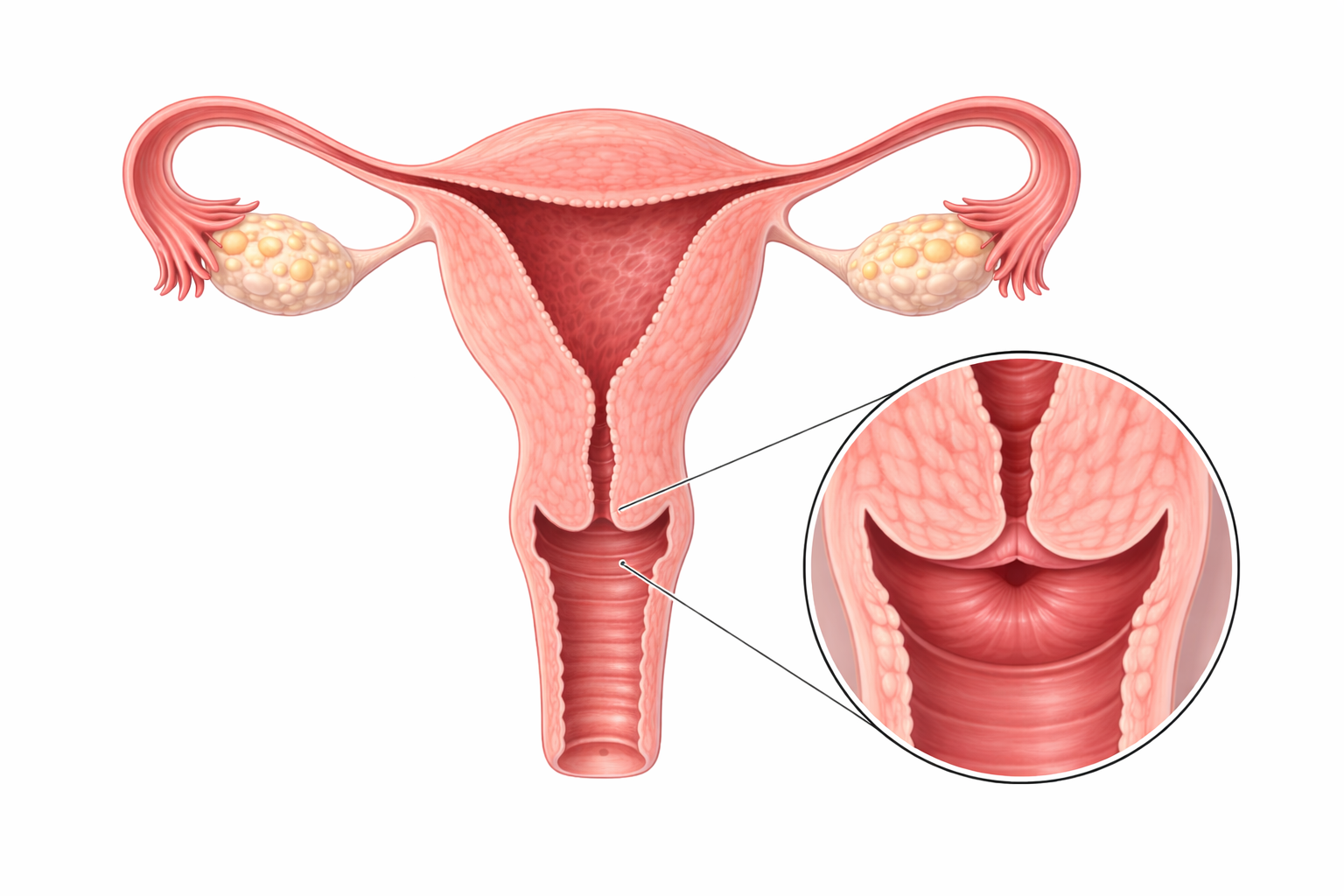
Image: The cervix is the lower, narrow part of the uterus that connects to the vaginal cannel.
Beyond the Basics
HPV Infection and Viral Persistence
Human papillomavirus (HPV) is transmitted through direct skin-to-skin contact and gains access to the cervix through microscopic abrasions in the epithelium. These small disruptions expose the basal epithelial cells, which are the only cells capable of sustained division and therefore support viral replication. In most individuals, the immune system recognises and clears the infection within months, often without symptoms.
Cervical cancer risk arises when high-risk HPV types persist rather than being cleared. Persistence allows viral DNA to integrate into the host cell genome, meaning the virus becomes part of the cell’s genetic material rather than existing independently. This integration leads to continuous expression of viral genes that interfere with normal cellular regulation, creating a long-term disruption of growth control rather than a transient infection.
Viral Oncoproteins and Loss of Cell-Cycle Control
High-risk HPV strains produce viral oncoproteins that directly interfere with tumour suppressor pathways. These tumour suppressor proteins normally act as checkpoints, regulating when a cell divides and triggering apoptosis (programmed cell death) if damage is detected.
When these regulatory systems are disrupted, cells no longer respond appropriately to signals that would normally limit proliferation or remove damaged cells. Instead, abnormal cells continue to divide, even in the presence of DNA damage. Over time, this leads to accumulation of mutations, genomic instability, and a progressive shift from controlled growth to uncontrolled proliferation.
Dysplasia and Stepwise Malignant Progression
Cervical cancer develops gradually through a series of identifiable precancerous stages, collectively referred to as dysplasia or cervical intraepithelial neoplasia (CIN). These changes reflect disordered epithelial maturation, where cells lose their normal structure, organisation, and differentiation as they move toward the surface.
Importantly, these abnormal cells remain confined above the basement membrane, which is the thin structural layer separating the epithelium from underlying tissue. This stage can persist for years, providing an opportunity for detection through screening. Progression to invasive cancer occurs when dysplastic cells breach the basement membrane, allowing access to stromal tissue, blood vessels, and lymphatics.
Local Invasion and Tissue Disruption
Once the tumour becomes invasive, malignant cells infiltrate surrounding cervical tissue and may extend into adjacent pelvic structures such as the uterus, vagina, or pelvic wall. As the tumour grows, it disrupts normal tissue architecture and compromises local blood vessels.
This process explains the clinical presentation. Fragile, abnormal blood vessels within the tumour are prone to bleeding, leading to symptoms such as postcoital bleeding or irregular vaginal bleeding. As invasion progresses, involvement of surrounding tissues and nerves contributes to pelvic pain and pressure, which are typically features of more advanced disease rather than early stages.
Lymphatic Spread and Regional Metastasis
The cervix has an extensive lymphatic network that provides a pathway for tumour spread once invasion has occurred. Malignant cells can enter lymphatic vessels and travel to regional lymph nodes, particularly those within the pelvis and para-aortic region. Lymphatic involvement reflects progression beyond local disease and is an important determinant of staging and prognosis. As tumour cells establish within lymph nodes, they may continue to proliferate and serve as a source for further spread, including distant metastasis.
Immune Evasion and Chronic Infection
Persistent HPV infection reflects a failure of immune clearance rather than simply increased viral aggressiveness. The virus employs several strategies to avoid detection, including limiting the expression of viral proteins in ways that reduce immune recognition and avoiding strong inflammatory responses that would otherwise recruit immune cells.
This ability to evade the immune system allows infected cells to survive and continue proliferating over time. It also explains why individuals with impaired immune function are at higher risk of persistent infection and progression to cancer. The effectiveness of HPV vaccination lies in preventing initial infection with high-risk strains, thereby interrupting this process before persistence and cellular disruption can occur.
Clinical Connections
Early cervical cancer is often asymptomatic, which is why it is frequently detected through screening rather than clinical presentation. As disease progresses, symptoms begin to reflect local tissue invasion and vascular disruption, rather than the presence of early cellular changes.
When symptoms do occur, they typically relate to tumour effects on surrounding structures:
abnormal vaginal bleeding, particularly postcoital or intermenstrual, due to fragile tumour vasculature
persistent or unusual vaginal discharge, sometimes watery or blood-stained
pelvic pain or pressure, indicating deeper local invasion
dyspareunia, reflecting involvement of surrounding tissues
These features usually indicate disease beyond the pre-invasive stage, where dysplastic changes have already progressed to invasive cancer. This is why screening programs are designed to detect cellular abnormalities before symptoms develop, when intervention is most effective.
Prevention and management are closely linked to the underlying disease process. HPV vaccination reduces the risk of initial infection with high-risk viral strains, interrupting the pathway to persistent infection and malignant transformation. Screening identifies dysplastic changes confined to the epithelium, allowing removal of abnormal tissue before it breaches the basement membrane. Once invasion has occurred, management is guided by the extent of local spread and lymphatic involvement, with treatment ranging from local excision to combined surgical and oncological approaches depending on stage.
Concept Check
Why is the cervical transformation zone particularly vulnerable to HPV-related malignancy?
How does persistent HPV infection disrupt normal cell-cycle regulation?
Why does cervical cancer progress slowly over many years?
Why are early stages of cervical cancer often asymptomatic?
How does lymphatic spread influence staging and prognosis?