THE VAGINA: Structure & Function
he vagina is a muscular, collapsible canal forming the passageway between the cervix and the external genitalia. Though often described simply as a birth canal or site of intercourse, the vagina is a highly specialised structure with dynamic physiological roles in protection, sexual function, and reproductive health. Its epithelial lining, microbiome, vascular network and muscular layers work together to maintain a resilient and responsive environment. Understanding vaginal structure and function is essential in reproductive anatomy, sexual health, gynaecology and obstetric practice, as well as in understanding how hormones, microbiota and physiological states influence the reproductive tract.
What You Need to Know
The vagina is a highly adaptable fibromuscular canal that functions as a conduit for menstruation, sexual intercourse, and childbirth while also playing a critical role in local immune defence. It is lined by non-keratinised stratified squamous epithelium, a tissue well suited to resist friction and mechanical stress. This epithelium can undergo significant stretching without injury, allowing the vaginal canal to accommodate both penetration and the passage of the fetus during birth.
Beneath the epithelial surface lies a richly vascular lamina propria and a muscular wall composed of interlacing smooth muscle fibres. This structural organisation provides both elasticity and tone, enabling the vagina to maintain its shape at rest while expanding when required. The surrounding connective tissue integrates the vagina with pelvic floor structures, supporting continence and contributing to pelvic stability.
The vaginal environment is tightly regulated and largely hormone dependent. Estrogen stimulates epithelial cells to accumulate glycogen, which is released as cells desquamate. This glycogen serves as a substrate for lactobacilli, dominant members of the normal vaginal microbiota. Through glycogen metabolism, lactobacilli produce lactic acid, maintaining an acidic vaginal pH that suppresses pathogenic organisms and supports microbial balance. Key features of normal vaginal physiology include:
Acidic pH, which provides protection against infection
Estrogen-dependent epithelial maturation, supporting microbial stability
Dynamic lubrication, enabling comfort and tissue protection
Vaginal lubrication arises primarily from transudation of plasma through the vaginal epithelium during sexual arousal, rather than from glandular secretion. This process is supplemented by mucus from the cervix and secretions from the vestibular glands. Together, these mechanisms allow the vagina to function as a resilient, self-regulating structure that balances protection, flexibility, and reproductive function across the lifespan.
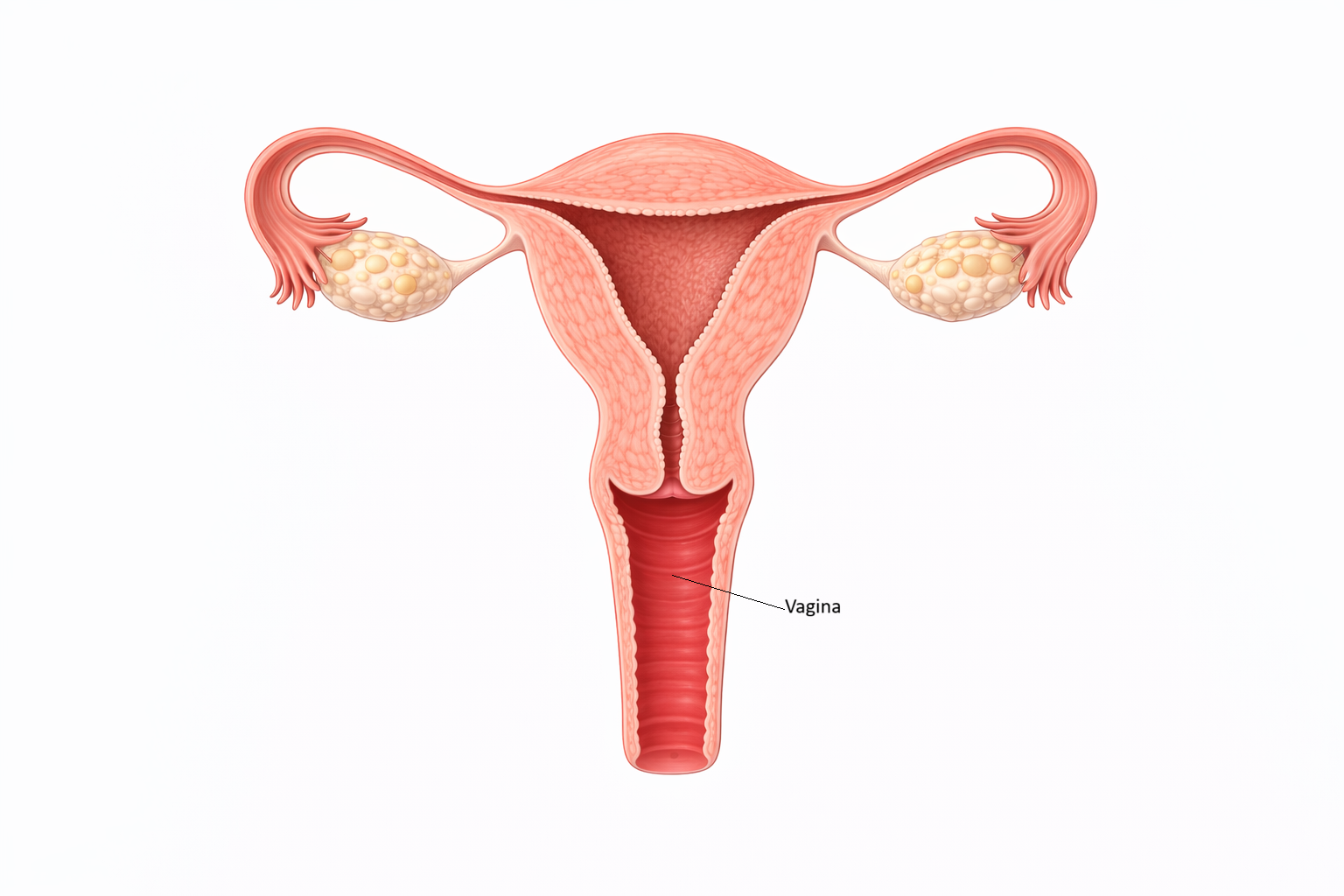
Image: The vagina is a fibromuscular canal extending from the cervix to the external genitalia, forming the lower portion of the female reproductive tract. It functions as the passage for menstrual flow, receives sperm during intercourse, and serves as the birth canal during labour, with its rugae allowing for significant distension.
Beyond the Basics
Anatomical Structure and Regional Features
The vagina is a distensible canal that typically measures around 8 to 10 cm in length, although this varies with age, hormonal status, and parity. It lies at an angle to the uterus and surrounds the cervix, forming anterior, posterior, and lateral fornices that allow close anatomical integration with the cervix and uterus. The vaginal epithelium is arranged into transverse folds known as rugae, which permit substantial expansion during sexual activity and childbirth while maintaining tissue integrity at rest.
Beneath the epithelium, the lamina propria contains elastic fibres, a dense vascular network, and lymphoid tissue that supports flexibility, tissue nutrition, and immune defence. The muscular layer consists of inner circular and outer longitudinal smooth muscle fibres, providing tone and limited contractile ability. An outer adventitial layer anchors the vagina to adjacent pelvic structures, including the bladder, urethra, and rectum, allowing mobility while maintaining positional stability. The absence of glands within the vaginal wall means lubrication depends on vascular transudation and cervical secretions rather than intrinsic glandular output.
Microenvironment and the Vaginal Microbiome
The vaginal microenvironment is a hormonally regulated ecosystem designed to balance protection with reproductive function. Estrogen stimulates epithelial cells to accumulate glycogen, which is released as cells desquamate. Lactobacillus species metabolise this glycogen into lactic acid, maintaining a low vaginal pH that limits growth of pathogenic organisms and supports microbial stability.
Beyond acid production, lactobacilli contribute additional protective mechanisms through secretion of hydrogen peroxide, bacteriocins, and biosurfactants that inhibit competing microbes. Shifts in estrogen exposure across the lifespan, including puberty, pregnancy, menopause, or hormonal contraception, alter epithelial thickness, glycogen availability, and microbial composition. Disruption of this balance increases susceptibility to conditions such as bacterial vaginosis and ascending genital tract infection, with broader implications for reproductive and obstetric health.
Hormonal Influence and Cyclical Variation
Estrogen plays a central role in maintaining vaginal structure and function. During the reproductive years, estrogen supports a thick, well-vascularised epithelium with high glycogen content and adequate lubrication. Across the menstrual cycle, estrogen-dominant phases favour epithelial resilience, increased moisture, and a vaginal environment more permissive to sperm survival.
Following menopause, declining estrogen leads to epithelial thinning, reduced glycogen stores, decreased lubrication, and a rise in vaginal pH. These changes underlie symptoms such as dryness, irritation, and dyspareunia and reflect physiological atrophy rather than primary infection. Hormonal modulation of vaginal tissue explains why local estrogen therapy can restore epithelial integrity and microbial balance in symptomatic individuals.
Vaginal Physiology in Sexual Function and Childbirth
During sexual arousal, increased pelvic blood flow enhances vascular engorgement and promotes transudation of fluid across the vaginal epithelium, resulting in lubrication. This response is coordinated through integrated parasympathetic, sympathetic, and somatic neural pathways that regulate vascular tone, muscle relaxation, and sensory input. The vaginal canal lengthens and expands, accommodating penetration while minimising tissue trauma.
In childbirth, the vagina demonstrates extraordinary adaptability. Its rugae, elastic fibre content, and collagen arrangement allow marked distension without permanent structural damage. The cervicovaginal junction plays a key role in directing the fetal head during descent, while coordinated pelvic floor relaxation facilitates delivery.
Local Immunity and Barrier Function
The vagina functions as an active immunological barrier rather than a passive conduit. Vaginal epithelial cells express pattern-recognition receptors that detect microbial threats and trigger local immune responses. Antimicrobial peptides, cytokines, and secretory immunoglobulin A contribute to mucosal defence while preserving tolerance to sperm during the fertile window.
This finely balanced immune environment allows the vagina to protect against infection while remaining responsive to reproductive demands. Disruption of immune regulation, whether through hormonal change, microbiome imbalance, or tissue injury, can compromise this barrier and increase vulnerability to infection and inflammation.
Clinical Connections
Changes in vaginal structure or microenvironment often present with symptoms that reflect disruption of hormonal support, microbial balance, or pelvic support rather than isolated local disease. Reduced estrogen exposure, particularly after menopause, leads to thinning of the vaginal epithelium, reduced lubrication, and a rise in vaginal pH. This state, often referred to as vaginal atrophy, increases susceptibility to irritation, recurrent infection, and sexual discomfort, and reflects physiological change rather than infection alone.
Disruption of the vaginal microbiome is another common source of clinical concern. Antibiotic use, hormonal fluctuations, and changes in sexual practices can reduce lactobacilli dominance, allowing overgrowth of anaerobic organisms. Bacterial vaginosis is characterised by loss of acidic pH, altered discharge, and increased risk of ascending infection. The clinical consequences of microbiome imbalance may include:
Recurrent vaginal symptoms, such as discharge, irritation, or odour related to altered microbial composition
Increased infection risk, including pelvic inflammatory disease and adverse pregnancy outcomes
Reduced mucosal defence, due to loss of lactobacilli and antimicrobial activity
Vaginal structure is closely linked to pelvic floor integrity. Weakness or injury to pelvic floor muscles and connective tissue can alter vaginal support, contributing to prolapse or urinary incontinence. Vaginal birth may stretch or injure muscular and fascial supports, sometimes leading to long-term changes in vaginal tone or elasticity. These effects vary widely and depend on factors such as tissue integrity, birth mechanics, and recovery of pelvic floor function.
Knowledge of anatomy of the vagina also informs contraception methods. Barrier methods rely on the vagina as a site of sperm containment, while pH-modifying agents exploit the sensitivity of sperm to acidic environments. Hormone delivery systems that act locally within the vagina influence epithelial thickness, lubrication, and microbial balance. Linking symptoms and interventions back to normal vaginal structure and function allows clinicians to distinguish physiological variation from pathology and tailor management accordingly.
Concept Check
How does estrogen influence the structure and function of the vaginal epithelium?
Why is the vaginal pH typically acidic, and what maintains this acidity?
How do rugae contribute to the mechanical properties of the vagina?
What hormonal changes contribute to vaginal atrophy after menopause?
How do lactobacilli contribute to local immunity within the vaginal canal?