THE CERVIX: Structure & Function
The cervix is the lower, cylindrical portion of the uterus that projects into the vagina and forms the gateway between the upper and lower reproductive tracts. Although often overshadowed by the uterus and ovaries, the cervix performs essential functions throughout the menstrual cycle, during pregnancy and at childbirth. Its unique combination of dense connective tissue, specialised epithelium and hormonally responsive mucus allows it to regulate fertility, protect the reproductive tract from infection and maintain pregnancy until term. Understanding the cervix requires an appreciation of both its structural rigidity and its remarkable capacity for remodelling. This dual nature is central to its roles in sperm transport, barrier function and cervical dilation during labour.
What You Need to Know
The cervix is a specialised structure that forms the lower portion of the uterus and plays a key role in fertility, pregnancy maintenance, and protection of the upper reproductive tract. Structurally, it is composed predominantly of dense, collagen-rich connective tissue with relatively small amounts of smooth muscle. This composition gives the cervix firmness and tensile strength, allowing it to remain closed for most of the reproductive cycle and throughout pregnancy while still being capable of remodelling when required.
Anatomically, the cervix is divided into two distinct regions with different epithelial linings and functions. The ectocervix projects into the vagina and is covered by stratified squamous epithelium, providing resilience against mechanical stress and the acidic vaginal environment. The endocervical canal connects the uterine cavity to the vagina and is lined by columnar epithelium containing mucus-secreting glands. The junction between these two epithelia, known as the transformation zone, is an area of active cellular change and has particular clinical significance.
Cervical function is highly responsive to hormonal fluctuations across the menstrual cycle. Estrogen and progesterone regulate the quantity and physical properties of cervical mucus, allowing the cervix to alternate between facilitating and restricting passage through the cervical canal. Key hormone-driven changes include:
Estrogen-dominant phases, when cervical mucus becomes thin, hydrated, and organised into channels that support sperm transport
Progesterone-dominant phases, when mucus thickens and becomes less permeable, limiting sperm entry and reducing pathogen ascent
Pregnancy-related changes, where sustained progesterone exposure leads to formation of a dense mucus plug that seals the cervical canal
Through these dynamic structural and biochemical adaptations, the cervix functions as both a gateway for reproduction and a protective barrier, balancing accessibility with security across the reproductive lifespan.
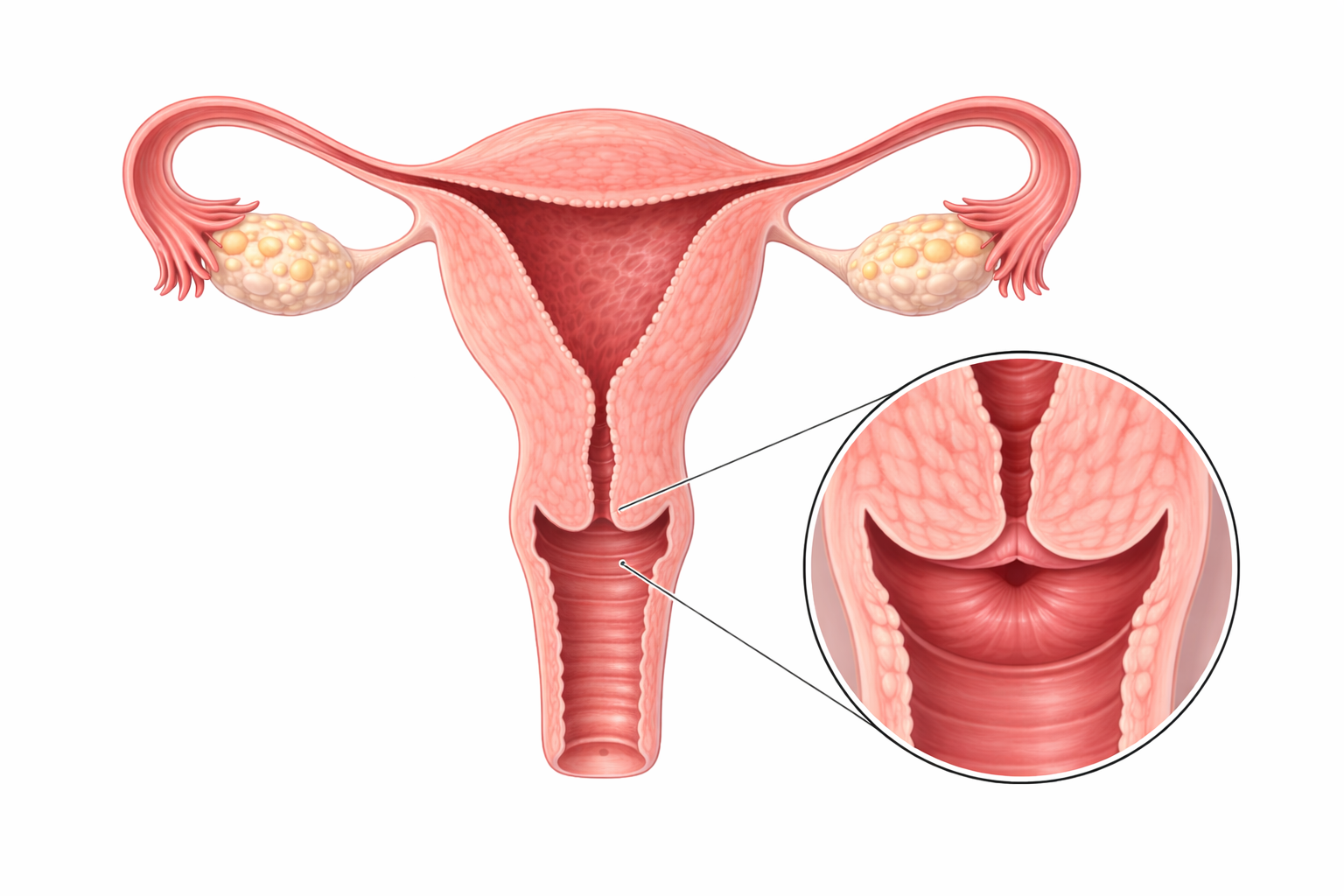
Image: The cervix is the lower portion of the uterus that connects the uterine cavity to the vaginal canal via the cervical canal. It acts as a functional gateway, allowing menstrual flow to exit, facilitating sperm entry, and undergoing structural changes during pregnancy and labour.
Beyond the Basics
Detailed Anatomy and Cervical Microstructure
The cervical stroma is built for strength rather than contraction. It is composed predominantly of type I and type III collagen fibres arranged in a dense, interwoven matrix that provides rigidity and resistance to mechanical stress. This collagen-rich framework allows the cervix to remain firm and closed throughout most of the menstrual cycle and for the duration of pregnancy. Small bundles of smooth muscle are present, particularly near the junction with the uterine body, but they contribute only limited contractile function compared with the myometrium.
The epithelial lining differs markedly across cervical regions and reflects functional demands. The ectocervix is covered by non-keratinising stratified squamous epithelium, which tolerates friction and exposure to the vaginal environment. In contrast, the endocervical canal is lined by tall columnar epithelial cells arranged into deep branching crypts that produce cervical mucus. The junction between these epithelia, known as the transformation zone, is a dynamic region where columnar cells are gradually replaced by squamous cells through metaplasia. This high cellular turnover explains why the transformation zone is the most common site for cervical dysplasia and malignant change.
Hormonal Regulation of Cervical Mucus
Cervical mucus is a hormonally responsive secretion that plays an active role in regulating fertility. During the late follicular phase, rising estrogen levels stimulate increased mucus production. The mucus becomes clear, hydrated, and stretchable, a property often described as spinnbarkeit. At a microscopic level, mucin glycoproteins align into parallel channels that protect sperm, support motility, and facilitate passage through the cervical canal.
After ovulation, progesterone induces a rapid shift in mucus composition. Water content decreases, viscosity increases, and the mucus becomes dense and adhesive. This change restricts sperm penetration and enhances antimicrobial defence, effectively closing the cervix during the luteal phase. These predictable hormone-driven changes form the physiological basis of fertility awareness methods and explain why the cervix alternates between permeability and protection across the cycle.
Cervical Function During Pregnancy
Throughout pregnancy, the cervix must maintain structural integrity while supporting increasing uterine weight. Progesterone promotes collagen cross-linking within the cervical stroma, reinforcing tissue strength and preventing premature dilation. At the same time, sustained progesterone exposure maintains the cervical mucus plug, a dense barrier that seals the endocervical canal and limits ascending infection.
As term approaches, the cervix undergoes a gradual process of ripening. Collagen fibres become disorganised and partially degraded, tissue hydration increases, and inflammatory mediators soften the stroma. These changes reduce cervical rigidity and allow dilation in response to coordinated uterine contractions. Inadequate cervical ripening can contribute to prolonged or obstructed labour, while premature softening may lead to cervical insufficiency and preterm birth.
Immune Defence and Barrier Protection
The cervix functions as an immunological interface between the external environment and the uterine cavity. Endocervical mucus contains immunoglobulins, lysozyme, and antimicrobial peptides such as defensins, providing continuous local immune surveillance. This defence is particularly important during phases when the cervix is more permeable to sperm.
The transformation zone remains especially vulnerable to infection due to its exposed basal cells and high rate of cellular turnover. Human papillomavirus preferentially infects this region, which explains the strong association between transformation zone pathology and cervical cancer. Understanding the cervix as both a structural barrier and an active immune organ highlights why screening and vaccination strategies are so effective in reducing cervical disease.
Clinical Connections
Pathology affecting the cervix has wide-reaching consequences for fertility, pregnancy outcomes, and long-term gynaecological health. Because cervical integrity depends on collagen structure, hormonal responsiveness, and immune defence, disruption in any of these systems can lead to clinically significant problems rather than isolated local symptoms.
Cervical insufficiency reflects failure of the cervical stroma to maintain rigidity during pregnancy, often due to altered collagen composition or premature remodelling. This can result in painless cervical dilation, second-trimester pregnancy loss, or preterm birth. Management strategies such as cervical cerclage or progesterone therapy aim to reinforce mechanical support or stabilise cervical tissue rather than treating uterine activity itself. Other structural abnormalities, such as cervical stenosis, may impede menstrual outflow or interfere with sperm passage, contributing to dysmenorrhoea, infertility, or difficulty with assisted reproductive procedures. Clinically relevant cervical dysfunction may present as:
Pregnancy complications, including mid-trimester loss or preterm birth related to cervical insufficiency
Fertility challenges, due to impaired mucus function or mechanical obstruction
Menstrual abnormalities, particularly with cervical narrowing or scarring
The transformation zone of the cervix is central to preventive care. Cervical screening targets this region because it is the primary site where dysplasia develops. Persistent infection with high-risk human papillomavirus is the underlying cause of most cervical cancers, making HPV vaccination one of the most effective cancer prevention strategies in clinical practice. Chronic cervicitis or repeated infection can also alter mucus composition and local immunity, reducing sperm viability and increasing susceptibility to ascending infection.
Progesterone-dominant contraception thickens cervical mucus, creating a physical and biochemical barrier that limits sperm entry even when ovulation suppression is incomplete. Linking symptoms, screening strategies, and treatment effects back to cervical structure and function allows clinicians to assess risk, guide prevention, and manage reproductive health with greater precision across the lifespan.
Concept Check
How do the epithelial linings of the ectocervix and endocervical canal differ, and why is this important?
What hormonal changes cause cervical mucus to shift from sperm-friendly to sperm-restrictive?
Why is the transformation zone a key area in cervical cancer screening?
How does cervical tissue change during pregnancy, and what is the purpose of the mucus plug?
What structural and biochemical changes occur during cervical ripening near term?