The Respiratory System - Overview
Disclosure: This article may contain affiliate links. If you purchase through these links, The Nurse Brain may earn a small commission at no extra cost to you. Only trusted resources for nursing education are recommended.
The respiratory system works closely with the cardiovascular system to enable gas exchange, ensuring that oxygen enters the bloodstream and carbon dioxide is removed. Four key processes facilitate respiration: pulmonary ventilation (breathing), external respiration (gas exchange between the alveoli and capillaries), transport of respiratory gases, and internal respiration (gas exchange between the blood in the capillaries and body tissues).
What You Need to Know
The respiratory system is divided into two main parts:
Upper airways: nares, nasal cavity, pharynx, and larynx
Lower airways: trachea, bronchi, bronchioles, and alveoli
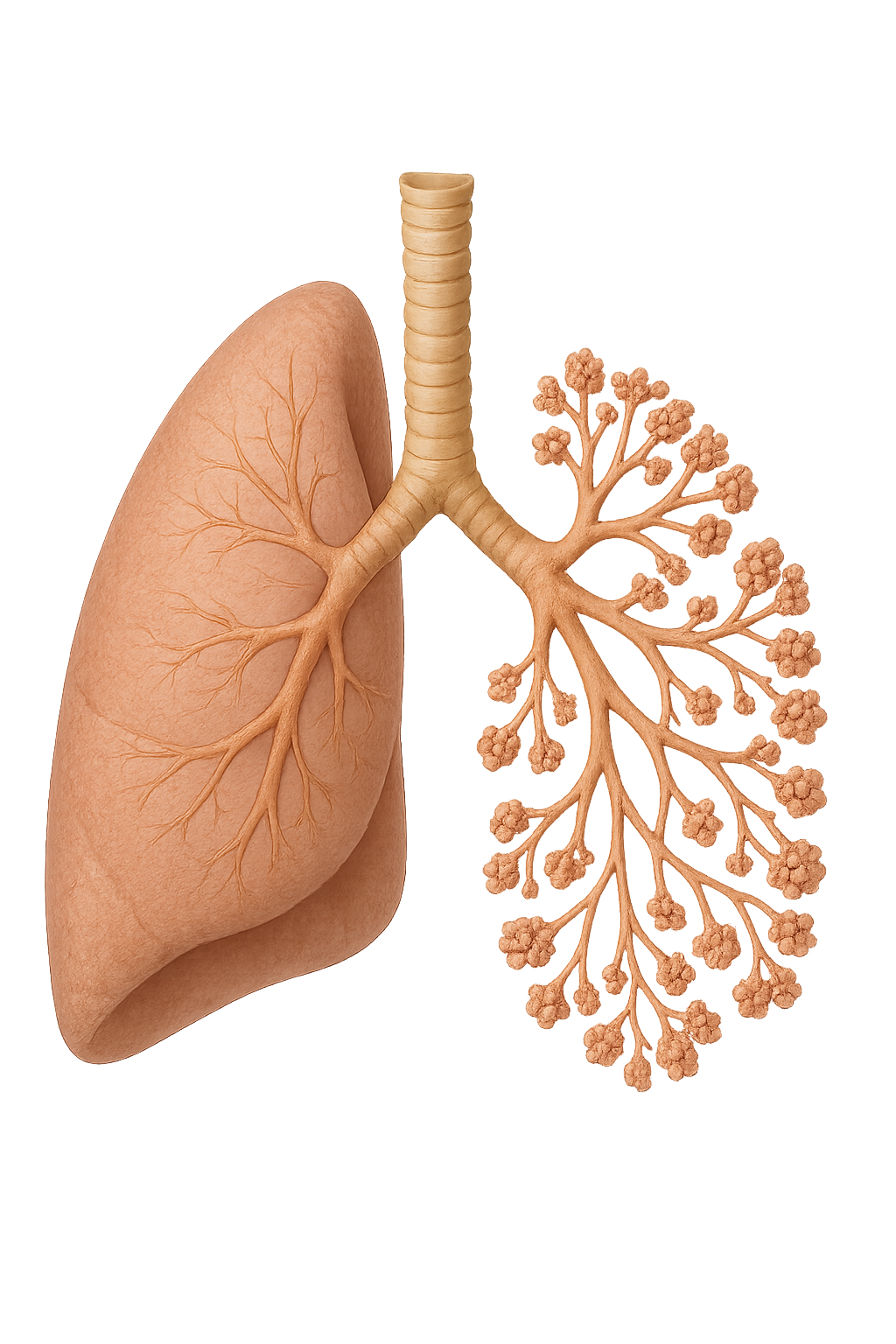
The trachea bifurcates (branches) into the right and left main bronchi, each entering a lung. These bronchi continue to branch into progressively smaller bronchioles, which ultimately terminate in clusters of alveoli—the functional units of the lungs where gas exchange occurs.
This branching structure, often referred to as the respiratory tree due to its resemblance to an upside-down tree, provides a large surface area to maximise gas exchange efficiency. Importantly, gas exchange only occurs within the alveoli. The trachea, bronchi, and bronchioles are therefore referred to as dead space, as no gas exchange takes place within these airways.
Now let’s look at some of the structures of the respiratory system in a bit more detail.
The Trachea, Bronchi and Bronchioles
The trachea sits in the midline of the neck and chest and anterior to the oesophagus. The trachea bifurcates (divides) distally at the larynx and at a point known as the carina. Structurally, the trachea is made up of 16-20 C-shaped hyaline cartilage rings, stacked vertically (on top of each other) with a thin membrane in between. The cartilage rings prevents collapse of the trachea. The open part of the “C”, situated posteriorly and facing the oesophagus, is made of smooth muscle and allows for expansion of the oesophagus into the trachea without obstructing the airway, as well as movement of the trachea during breathing, coughing and speaking.
The right main bronchus is wider, shorter and more vertical (straighter) than the left bronchus due to the position of the heart lying toward the left of the chest cavity. This is why inhaled objects are more likely to be lodged in the right bronchus. Bronchi are made of cartilage and smooth muscle.
The bronchi further divide in the lungs into secondary (lobar) and tertiary (segmental) bronchi. Tertiary bronchi branch off into bronchioles, smaller airways roughly 1mm in diameter. Unlike bronchi, bronchioles are made only of smooth muscle, not cartilage. Bronchioles continue to divide into smaller branches- terminal bronchioles and respiratory bronchioles, which connect to alveolar ducts and alveoli, where gas exchange occurs.
The Lungs, Pleura and Alveoli
The lungs, located in the thoracic cavity, have a spongy, elastic texture that allows for expansion and contraction during respiration.
The right lung has three lobes - (right upper lobe (RUL), right middle lobe (RML) and right lower lobe (RLL)). The left lung has two lobes and a cardiac notch, which makes space for the heart (left upper lobe and left lower lobe).
Each lung is encased in a pleural membrane comprised of two layers:
Visceral Pleura – covers the lung surface
Parietal Pleura – lines the thoracic wall
A thin layer of pleural fluid lies between these layers, allowing the lungs to move smoothly (without friction or pain) during breathing.
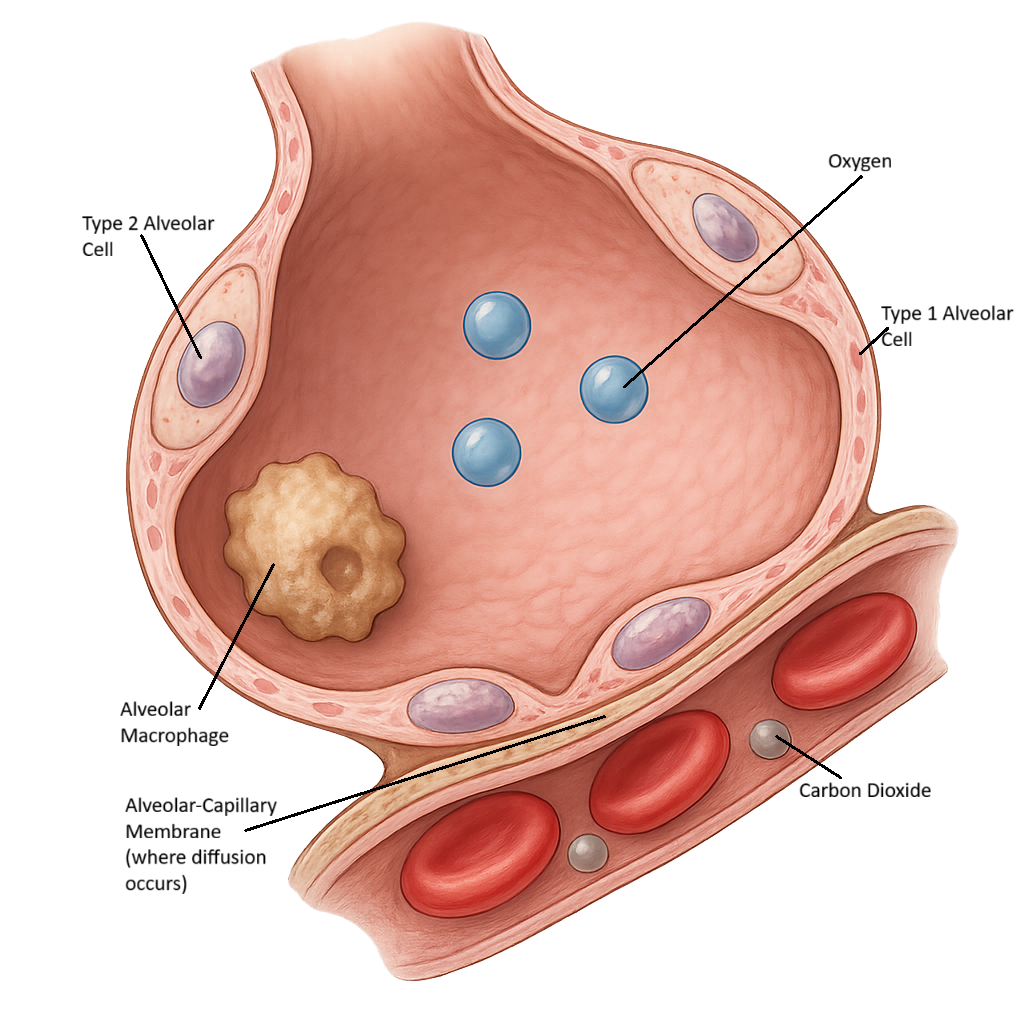
Alveoli are tiny, balloon-like air sacs located at the terminal ends of bronchioles. They are the functional unit of the lungs and share a thin interface with pulmonary capillaries. This interface is where gas exchange occurs – carbon dioxide diffuses from the blood in the capillaries into the alveoli and oxygen diffuses from the alveoli into the blood in the capillaries. Multiple capillaries surround each alveolus. This dense pulmonary capillary bed maximises the surface area for gas exchange.
The alveolar wall is extremely thin – about 0.2 to 0.5 micrometres thick and is comprised of:
Type I alveolar cells (pneumocytes) - these cells are specialised for rapid diffusion of gases.
Type II alveolar cells - which secrete pulmonary surfactant, a lipid-rich substance that reduces surface tension and alveolar collapse.
The alveolar wall also contains alveolar macrophages – a mobile immune cell that patrols and destroys inhaled dust, debris and pathogens. Between each alveolar are alveolar pores, or openings, which help to maintain pressure equalisation and even inflation of the lungs.
Beyond the Basics
The respiratory system does more than just exchange gases — it also protects itself from infection and debris through a range of protective mechanisms. These include the mucociliary escalator, the cough reflex, and immune defences, which work together to keep the airways clear and the lungs pathogen-free. Let’s explore how each of these mechanisms contributes to respiratory protection.
Mucociliary Escalator
The mucociliary escalator is a key defence mechanism of the respiratory tract. It consists of mucus and cilia, which line the respiratory epithelium. The cilia are microscopic, hair-like projections that beat in a coordinated, wave-like motion to move mucus upward toward the pharynx. The mucus layer traps dust, microorganisms, and other airborne particles, while the ciliary movement propels this debris out of the lungs to be coughed up or swallowed.
Beneath the mucus is a thin layer of periciliary fluid (or sol layer), which allows the cilia to beat freely. This fluid has a carefully balanced composition of water and electrolytes, such as sodium, chloride, and bicarbonate ions, which help maintain the optimal viscosity and pH for ciliary function. When this balance is disrupted — for example, due to dehydration, infection, or smoking — mucociliary clearance becomes less effective, increasing the risk of respiratory infection.
Cough Reflex
The cough reflex clears irritants, mucus, and foreign material from the respiratory tract. It is initiated when sensory receptors in the airway detect mechanical or chemical stimuli, such as dust, smoke, or excess mucus.
Two main types of receptors are involved:
Rapidly adapting receptors (RARs): Located primarily in the trachea and bronchi, these respond to sudden changes like mechanical irritation or mucus accumulation.
C-fibre receptors (or nociceptors): Found throughout the airways, these are activated by chemical irritants such as capsaicin, inflammatory mediators, or noxious gases.
When activated, these receptors send afferent impulses via the vagus nerve (cranial nerve X) to the cough centre in the medulla oblongata. The medulla integrates the sensory input and triggers a coordinated motor response through efferent pathways involving the phrenic nerve, spinal motor nerves, and recurrent laryngeal branch of the vagus nerve.
This produces the characteristic cough sequence:
Deep inspiration to fill the lungs.
Closure of the glottis and contraction of the respiratory muscles (diaphragm, intercostals, and abdominal muscles), building high intrathoracic pressure.
Sudden opening of the glottis, propelling air out forcefully to expel mucus or foreign matter.
The cough reflex is vital for maintaining airway patency and preventing infection. Impairment of this reflex — such as through sedation, neurological injury, or prolonged intubation — increases the risk of mucus retention, aspiration, and respiratory complications.
Immune Defence
The respiratory system is constantly exposed to airborne microorganisms, allergens, and pollutants, so it relies on multiple layers of immune defence to prevent infection and maintain airway integrity. These defences can be divided into innate (non-specific) and adaptive (specific) components, which work together to identify, neutralise, and remove potential pathogens.
Innate immune defences provide the first line of protection and include:
Epithelial barriers: The cells lining the airways form tight junctions that prevent pathogen entry.
Mucus and antimicrobial substances: Mucus traps particles, while secretions such as lysozyme, lactoferrin, and defensins have antimicrobial activity.
Resident immune cells: Alveolar macrophages patrol the alveoli, engulfing and digesting pathogens and debris through phagocytosis. Neutrophils may also be recruited during infection to enhance clearance.
Pattern recognition receptors (PRRs): These receptors, found on epithelial and immune cells, detect common microbial structures and trigger inflammatory responses.
If pathogens bypass the innate barriers, the adaptive immune system provides a more targeted response. This involves:
Lymphocytes (T and B cells) in airway-associated lymphoid tissue, which recognise specific antigens.
Plasma cells that produce immunoglobulin A (IgA) antibodies secreted into the mucus. IgA binds to pathogens, preventing them from adhering to epithelial cells and marking them for removal.
Together, these mechanisms ensure the respiratory system remains a highly efficient and self-cleaning environment. When immune defences are compromised — as in chronic smoking, viral infection, or immunosuppression — the risk of respiratory infection and inflammation increases significantly.
Clinical Connections
The respiratory system protects itself through a combination of mechanical and immune defences that maintain airway patency and prevent infection. Adequate hydration is essential to maintain the periciliary fluid layer and support effective mucociliary clearance. Smoking, pollution, and dehydration can damage cilia, thicken mucus, and reduce clearance, increasing infection risk.
Key factors that impair airway defence:
Dehydration → thickened mucus and reduced ciliary function
Smoking and pollutants → ciliary damage and impaired clearance
Sedation or neurological impairment → reduced cough effectiveness
Immune suppression → increased susceptibility to infection
The cough reflex may be impaired in patients who are sedated, postoperative, or have neurological disorders, making them more prone to mucus retention and aspiration. Similarly, immune suppression from illness or medication weakens the body’s ability to fight respiratory infections.
These clinical relationships highlight the importance of interventions such as encouraging hydration and deep breathing, promoting early mobilisation, monitoring cough effectiveness, and educating patients about airway protection and smoking cessation. Supporting these natural defence mechanisms plays a vital role in maintaining healthy lung function and preventing respiratory complications.
Concept Check
A postoperative patient has a weak cough and thick secretions. Which respiratory protective mechanism is most compromised, and what interventions could support airway clearance?
How might smoking affect the mucociliary escalator and immune defences, and why does this increase infection risk?
Explain why hydration is important for maintaining effective airway clearance.
How does prolonged immobility contribute to impaired airway clearance, and what nursing interventions can reduce this risk?
Why are patients with neurological impairment at increased risk of aspiration, and how does this compromise normal respiratory defence mechanisms?