Upper Respiratory Tract Anatomy & Function
The upper respiratory tract forms the entry pathway for air and provides the first line of defence against pathogens, particles, and environmental irritants. Although often overshadowed by the lungs, this region plays several essential roles: warming and humidifying incoming air, filtering debris, facilitating smell and taste, and producing vocal sounds. Its protective epithelial lining, mucous production, and ciliary movement form a highly coordinated system that keeps the lower airways sterile and functioning optimally.
What You Need to Know
The upper respiratory tract includes the nasal cavity, paranasal sinuses, pharynx, and larynx. It functions as both a conduit for airflow and a critical conditioning and defence system. Before air reaches the lungs, it is filtered, warmed, humidified, and screened for harmful particles, protecting the delicate gas-exchange surfaces below.
Key functions of the upper respiratory tract:
Filter inhaled air and trap particles
Warm and humidify incoming air
Provide early immune defence
Direct airflow safely toward the lower airways
The nasal cavity is the primary entry point for inspired air. Its highly vascular mucosa warms air, while mucous secretions humidify it. The turbinates create turbulent airflow, increasing contact with the mucosa and improving filtration. Fine hairs and sticky mucus trap dust, microbes, and pollutants. The olfactory region also detects odours, acting as an early warning system for harmful substances.
The paranasal sinuses are air-filled cavities connected to the nasal cavity. They produce mucus that drains into the nasal passages, helping trap particles and maintain moisture. Narrow drainage pathways mean that swelling or thickened secretions can block outflow, leading to mucus accumulation and sinusitis.
The pharynx is a muscular tube linking the nasal cavity and mouth to the larynx and oesophagus. It is divided into the nasopharynx, oropharynx, and laryngopharynx, allowing it to manage both airflow and swallowing. Lymphoid tissue within the pharynx samples inhaled and ingested material, supporting early immune responses.
The larynx serves as a gateway to the lower respiratory tract. Its cartilaginous structure maintains airway patency, while the epiglottis prevents aspiration during swallowing. The vocal cords also enable sound production, making the larynx essential for airway protection, airflow regulation, and speech.
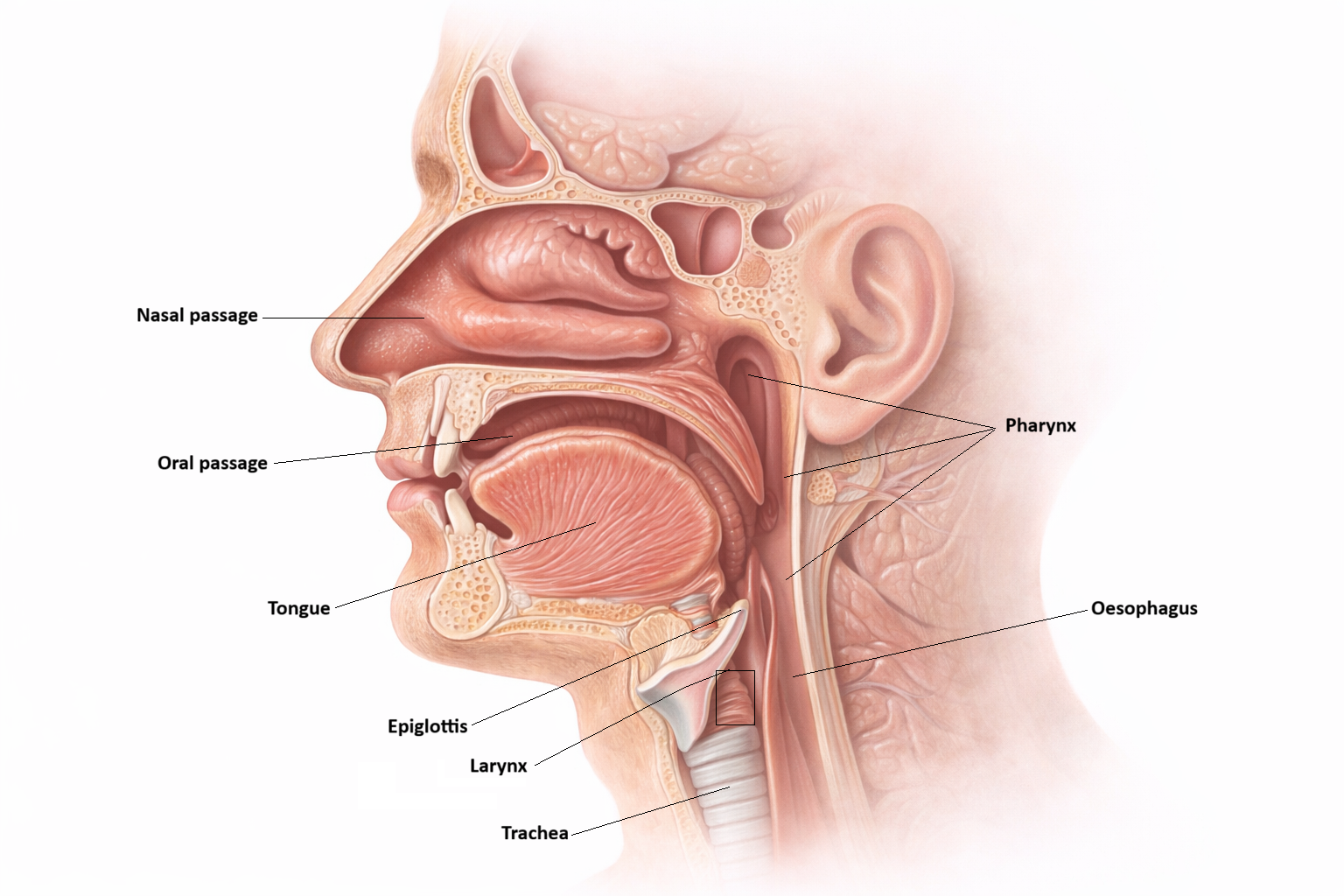
Image: Structures of the upper respiratory tract.
Beyond the Basics
Epithelial Specialisation in the Upper Airway
The upper airway is lined predominantly by pseudostratified ciliated columnar epithelium, a tissue type well suited to conditioning and protecting inspired air. This epithelium contains ciliated cells, mucus-secreting goblet cells, and basal cells that support epithelial renewal. Together, these components form an effective barrier against inhaled particles and microorganisms.
In regions exposed to greater mechanical stress, such as the oropharynx, the epithelium transitions to stratified squamous epithelium. This tissue sacrifices mucociliary function in favour of durability, providing protection against abrasion from food and swallowing. These regional differences reflect a balance between mechanical protection and airway defence.
The Mucociliary Escalator and Airway Clearance
Cilia within the upper airway beat in a highly coordinated, wave-like pattern that propels mucus toward the pharynx. This process, known as the mucociliary escalator, continuously clears trapped pathogens, dust, and debris from the respiratory tract, directing them toward the gastrointestinal system for elimination.
Effective mucociliary clearance depends on intact ciliary function and appropriately hydrated mucus. Smoking, dehydration, air pollution, and viral infections impair ciliary activity and alter mucus properties, slowing clearance. When this system is compromised, secretions accumulate, increasing susceptibility to infection and prolonging inflammatory processes within the airway.
Upper Airway Resistance and Work of Breathing
The upper airway contributes a substantial proportion of total airway resistance under normal conditions. Because airflow resistance is highly sensitive to changes in airway radius, even mild mucosal swelling can significantly increase resistance. This explains why conditions such as viral upper respiratory infections or allergic rhinitis can make breathing feel disproportionately difficult despite minimal anatomical narrowing.
Increased resistance in the upper airway raises the work of breathing and promotes mouth breathing, which bypasses normal air conditioning functions of the nasal passages. Over time, this can exacerbate lower airway irritation and dryness, further impairing respiratory efficiency.
Anatomical Continuity and Pressure Regulation
The upper airway is anatomically continuous with adjacent structures, including the paranasal sinuses and the middle ear. Drainage pathways and pressure-equalising connections mean that inflammation or obstruction in one region can affect others. For example, nasal congestion may impair sinus drainage or disrupt middle ear pressure regulation, contributing to conditions such as sinusitis or otitis media.
The larynx plays a critical protective role at the junction between the upper and lower airways. It contains highly sensitive receptors that detect foreign material and trigger protective reflexes, including coughing, breath-holding, and laryngospasm. These reflexes prevent aspiration and protect the lower respiratory tract, particularly during swallowing or exposure to irritants.
Integration of Upper Airway Structure and Function
The upper airway is not merely a conduit for airflow but an active participant in respiratory defence, airflow regulation, and airway protection. Its specialised epithelium, clearance mechanisms, resistance properties, and reflex pathways work together to maintain airway patency and protect the delicate gas-exchange surfaces below.
Disruption of any component, whether through inflammation, infection, or structural compromise, can have downstream effects on breathing efficiency and susceptibility to respiratory disease.
Clinical Connections
Upper respiratory tract disorders are among the most common problems encountered in clinical practice, but they can range from mild and self-limiting to rapidly life-threatening. Viral upper respiratory infections increase mucus production and damage ciliated epithelium, slowing mucociliary clearance and allowing secretions, bacteria, and inflammatory debris to accumulate. This explains why patients develop nasal congestion, sinus pressure, sore throat, and postnasal drip, and why secondary bacterial sinusitis or otitis media can follow a viral illness.
Allergic rhinitis represents immune-mediated inflammation of the nasal mucosa driven by IgE and histamine release. This causes vasodilation, tissue oedema, and excessive mucus secretion, leading to nasal obstruction, sneezing, itching, and watery discharge. Because airflow is disrupted and mucus clearance impaired, patients often develop sinus congestion, sleep disturbance, and recurrent infections.
Some upper airway conditions pose immediate threats to ventilation:
Epiglottitis causes rapid swelling of the epiglottis, risking sudden airway obstruction
Anaphylaxis produces diffuse mucosal oedema, bronchoconstriction, and stridor
Tonsillar hypertrophy or abscess can narrow the oropharynx and impair swallowing or breathing
These conditions require urgent recognition and escalation, as even small degrees of swelling in the upper airway can produce severe airflow limitation.
Laryngitis affects the vocal cords, leading to hoarseness and voice loss because inflamed or oedematous cords cannot vibrate normally. Chronic irritation from smoking or reflux leads to epithelial metaplasia, where ciliated respiratory epithelium is replaced by squamous epithelium (cells better suited to abrasion but unable to clear mucus). This structural change reduces airway defence, increases infection risk, and contributes to chronic cough and sputum retention.
Concept Check
What are the primary functions of the nasal turbinates?
Why is pseudostratified ciliated epithelium so important in the upper airway?
What mechanisms protect the lower airway from aspiration?
How does sinus drainage contribute to infection risk?
Why can mild mucosal swelling dramatically increase airflow resistance?