Blood Composition: Plasma, Cells & Proteins
Blood is a specialised connective tissue that plays a central role in transport, immunity, thermoregulation, and haemostasis. Its composition reveals enormous information about a person’s health, making blood tests essential in diagnosing disease. Blood contains both liquid and cellular components, each with highly specialised functions. Understanding what blood is made of, and how each component contributes to health, provides the foundation for interpreting full blood counts, recognising abnormalities, and understanding conditions such as anaemia, infection, inflammation, and clotting disorders.
What You Need to Know
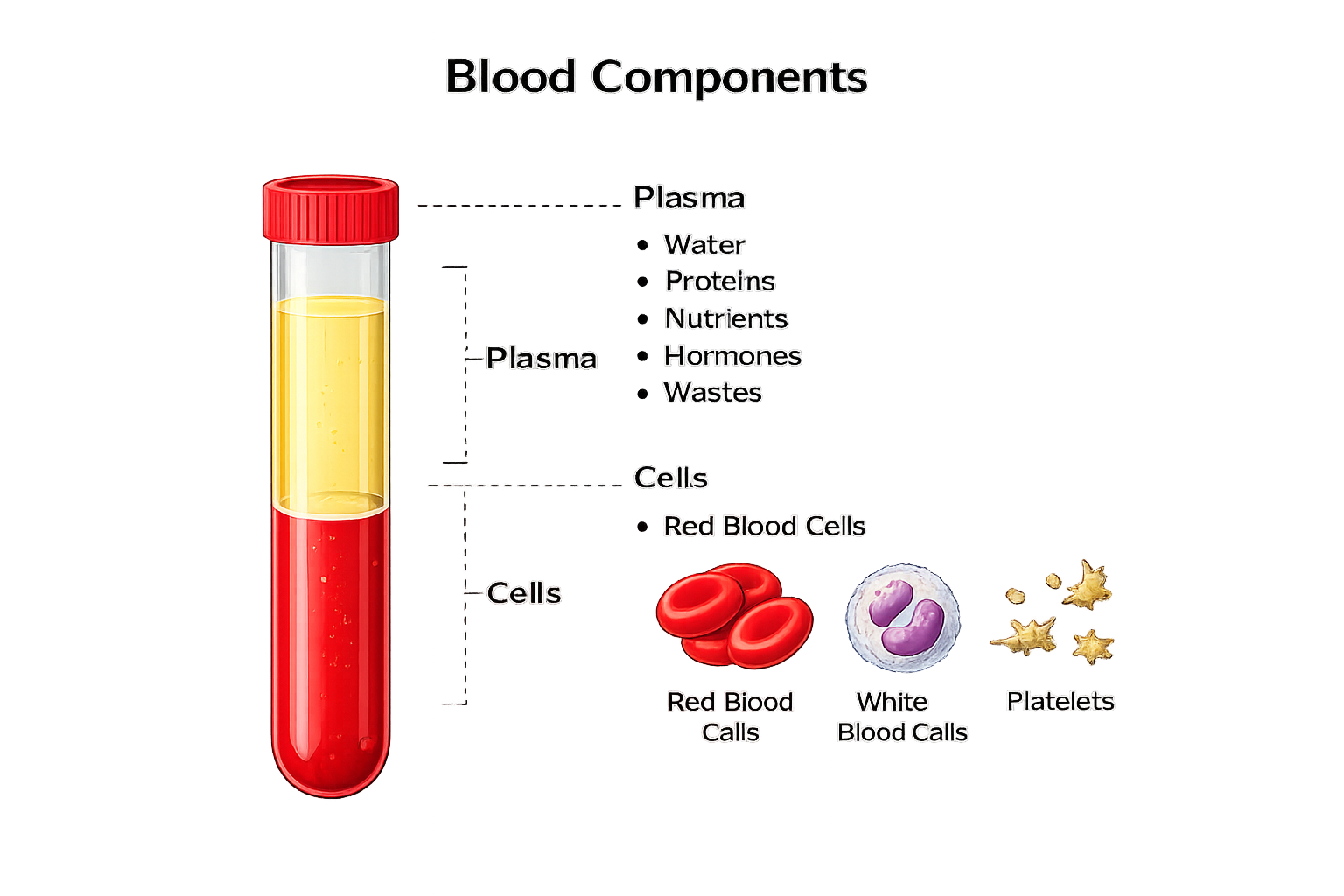
Blood consists of two main components: plasma and formed elements. Plasma makes up about 55% of total blood volume and is primarily water, giving it the ability to transport nutrients, electrolytes, hormones, waste products, and heat. Plasma also contains vital proteins, including albumin, which maintains oncotic pressure; globulins, which support immunity; and fibrinogen, essential for clotting. Plasma is primarily composed of:
water (90-92%)
plasma proteins (7-8%): albumnin, globulins, fibrinogen
dissolved solutes (1-2%): electrolytes, nutrients, hormones, waste products
The formed elements include red blood cells (erythrocytes), white blood cells (leukocytes), and platelets (thrombocytes). Red blood cells are the most numerous and contain haemoglobin, the protein responsible for oxygen transport. Their biconcave shape increases surface area for gas exchange and allows flexibility to navigate capillaries. White blood cells are key players in immunity and include neutrophils, lymphocytes, monocytes, eosinophils, and basophils, each with specific defensive roles. Platelets are small cell fragments responsible for the initial stages of clot formation, adhering to damaged vessels and activating the clotting cascade.
Beyond the Basics
Plasma Proteins and Fluid Balance
Plasma proteins are essential for maintaining the physical and chemical stability of blood. Albumin is the most abundant plasma protein and is the primary determinant of colloid osmotic pressure (pulls fluid back into the capillaries, which helps to maintain vascular volume and prevent oedema). By exerting an inward-pulling force within capillaries, albumin counterbalances hydrostatic pressure (drives fluid out of capillaries) and helps keep fluid within the intravascular space. This role is central to maintaining circulating volume and effective tissue perfusion.
Albumin also acts as a versatile transport protein. It binds a wide range of substances, including hormones, fatty acids, bilirubin, and many medications. This binding regulates the availability of these substances in the bloodstream and facilitates their delivery to target tissues. Changes in albumin concentration therefore influence not only fluid distribution but also the transport and bioactivity of circulating molecules.
Globulins and Circulating Defence Proteins
Globulins encompass a broad group of plasma proteins with diverse functions. Immunoglobulins form a major subgroup and provide specific immune defence by recognising and binding antigens. These proteins circulate continuously, allowing rapid immune responses when pathogens are encountered.
Other globulins serve as carrier proteins for lipids, metal ions, and fat-soluble vitamins. Together, these proteins support metabolic processes and contribute to the regulation of immune and inflammatory responses. The relative proportions of albumin and globulins are infuenced by the balance between nutritional status, immune activity, and protein synthesis.
Coagulation Factors in Plasma
Plasma contains numerous clotting factors that circulate in inactive forms under normal conditions. This arrangement allows the blood to remain fluid while retaining the capacity to clot rapidly when vascular injury occurs. Activation of these factors follows a tightly regulated sequence that localises clot formation to the site of injury.
Most clotting factors are synthesised in the liver, linking plasma coagulation capacity to hepatic function. Their presence in plasma ensures that haemostasis can be initiated immediately without the need for new protein synthesis, highlighting the importance of plasma as a functional reservoir rather than a passive medium.
Red Blood Cells and Erythrocyte Turnover
Red blood cells dominate the cellular component of blood and are specialised for oxygen transport. Their biconcave shape increases surface area and flexibility, optimising gas exchange and allowing passage through narrow capillaries. Haemoglobin within erythrocytes binds oxygen reversibly, enabling efficient delivery to tissues according to metabolic demand.
Erythropoiesis occurs continuously in the bone marrow and is regulated primarily by erythropoietin released from the kidneys in response to tissue oxygen levels. Mature red blood cells circulate for approximately 120 days before being removed by macrophages in the spleen and liver. Iron from degraded haemoglobin is conserved and recycled, supporting ongoing red cell production.
White Blood Cells and Immune Function
White blood cells comprise several distinct populations, each adapted to specific immune roles. Neutrophils provide rapid, short-term responses to infection, while monocytes migrate into tissues and differentiate into macrophages. Lymphocytes support adaptive immunity, with memory cells enabling long-lasting immune recognition.
The wide variation in white blood cell lifespan reflects functional diversity within the immune system. Some cells are designed for immediate defence and rapid turnover, while others persist for years to maintain immunological memory. This diversity allows the immune system to respond effectively to both acute and long-term challenges.
Platelets and Vascular Maintenance
Platelets are small, anucleate fragments (lack a nucleus) derived from megakaryocytes in the bone marrow. Their primary role is to preserve vascular integrity by rapidly adhering to sites of endothelial disruption. Once activated, platelets aggregate and release chemical mediators that support clot formation.
Although platelets circulate for only 7–10 days, their constant production maintains a ready supply. A proportion of circulating platelets is temporarily sequestered in the spleen, contributing to regulation of platelet numbers and availability within the bloodstream.
Dynamic Nature of Blood Composition
Blood composition is not static but adapts continuously to physiological conditions. Plasma volume, cellular concentration, and protein composition fluctuate in response to hydration status, immune activity, and long-term disease processes. These shifts alter the relative proportions of plasma and formed elements without necessarily changing total cell numbers.
Plasma proteins, red blood cells, white blood cells, and platelets function as an integrated system that supports oxygen delivery, immune defence, haemostasis, and fluid balance.
Clinical Connections
Abnormalities in blood composition produce some of the most common and clinically important presentations seen in healthcare. Because blood circulates through every organ, even subtle changes in its cellular or plasma components can cause widespread physiological effects.
Anaemia reduces oxygen delivery to tissues and typically presents with fatigue, pallor, exertional dyspnoea, dizziness, and tachycardia. In older adults or those with cardiac disease, even moderate anaemia may precipitate angina, heart failure, or syncope. In contrast, elevated haemoglobin or haematocrit increases blood viscosity, raising the risk of thrombosis, stroke, and myocardial infarction.
Changes in white blood cell counts provide critical diagnostic clues:
Leukocytosis often reflects infection, inflammation, trauma, or steroid use
Neutrophilia points toward bacterial infection
Lymphocytosis is common in viral illness
Leukopenia signals bone marrow suppression or severe sepsis and greatly increases infection risk
Platelet abnormalities have immediate bleeding or clotting implications. Thrombocytopenia may cause bruising, petechiae, mucosal bleeding, or intracranial haemorrhage, while excessive platelet activity contributes to thrombosis, myocardial infarction, and stroke.
Plasma proteins are equally important. Low albumin reduces plasma oncotic pressure, allowing fluid to leak into tissues and body cavities, producing oedema, ascites, and pleural effusions. Abnormal clotting factor levels, whether from liver disease, vitamin K deficiency, anticoagulant therapy, or genetic disorders, lead to either uncontrolled bleeding or inappropriate clot formation.
Blood composition also directly guides treatment decisions. Severe anaemia may require red cell transfusion to restore oxygen-carrying capacity. Thrombocytopenia with bleeding risk may require platelet transfusion. Plasma products are used to replace clotting factors in liver failure, massive haemorrhage, or warfarin reversal.
In clinical settings, nurses play a central role in this process by:
Verifying blood products and patient identity
Monitoring for transfusion reactions (fever, hypotension, rash, dyspnoea)
Assessing for bleeding, clotting, or fluid overload
Tracking trends in haemoglobin, white cells, platelets, and coagulation tests
Understanding blood composition allows early recognition of deterioration and safer, more effective patient care.
Concept Check
What are the main components of plasma, and why are they important?
How does the shape of a red blood cell support its function?
Which white blood cell types increase during bacterial infection?
Why does hypoalbuminaemia cause oedema?
What clinical signs might suggest thrombocytopenia?