Blood Vessels: Arteries, Veins and Capillaries
Blood vessels form the vast network that carries blood to and from every cell in the body. Although often taught as simple tubes, their structure is highly specialised to match their function. Arteries must withstand high pressures from the forceful ejection of blood from the heart. Veins, operating under much lower pressure, rely on valves and external muscle contraction to help return blood to the heart. Capillaries are the critical interface where oxygen, nutrients, hormones, and waste products are exchanged with tissues.
What You Need to Know
Arteries carry blood away from the heart and have thick, elastic walls designed to handle the high pressure of ventricular contraction. Their structure consists of three layers:
the tunica intima (inner lining)
tunica media (the muscular middle layer)
tunica externa (outer connective tissue)
The abundant smooth muscle and elastic fibres allow arteries to stretch and recoil, maintaining continuous forward blood flow even between heartbeats.
Veins return blood to the heart and have thinner walls and less muscular tissue, due to the much lower pressure within them. Because venous return depends largely on skeletal muscle contraction and pressure changes during breathing, veins contain one-way valves that prevent backflow. These valves are particularly important in the lower limbs, where blood must travel against gravity. When these valves fail, venous pooling and varicose veins may occur.
Capillaries are tiny, thin-walled vessels where exchange of gases, nutrients, and waste occurs. They consist of a single layer of endothelial cells resting on a basement membrane, allowing rapid diffusion. Their density in a tissue reflects metabolic demand, for example, skeletal muscle and cardiac muscle are rich in capillaries, whereas connective tissue contains fewer. The arrangement of capillaries enables efficient movement of substances between blood and interstitial fluid, supporting cellular metabolism.
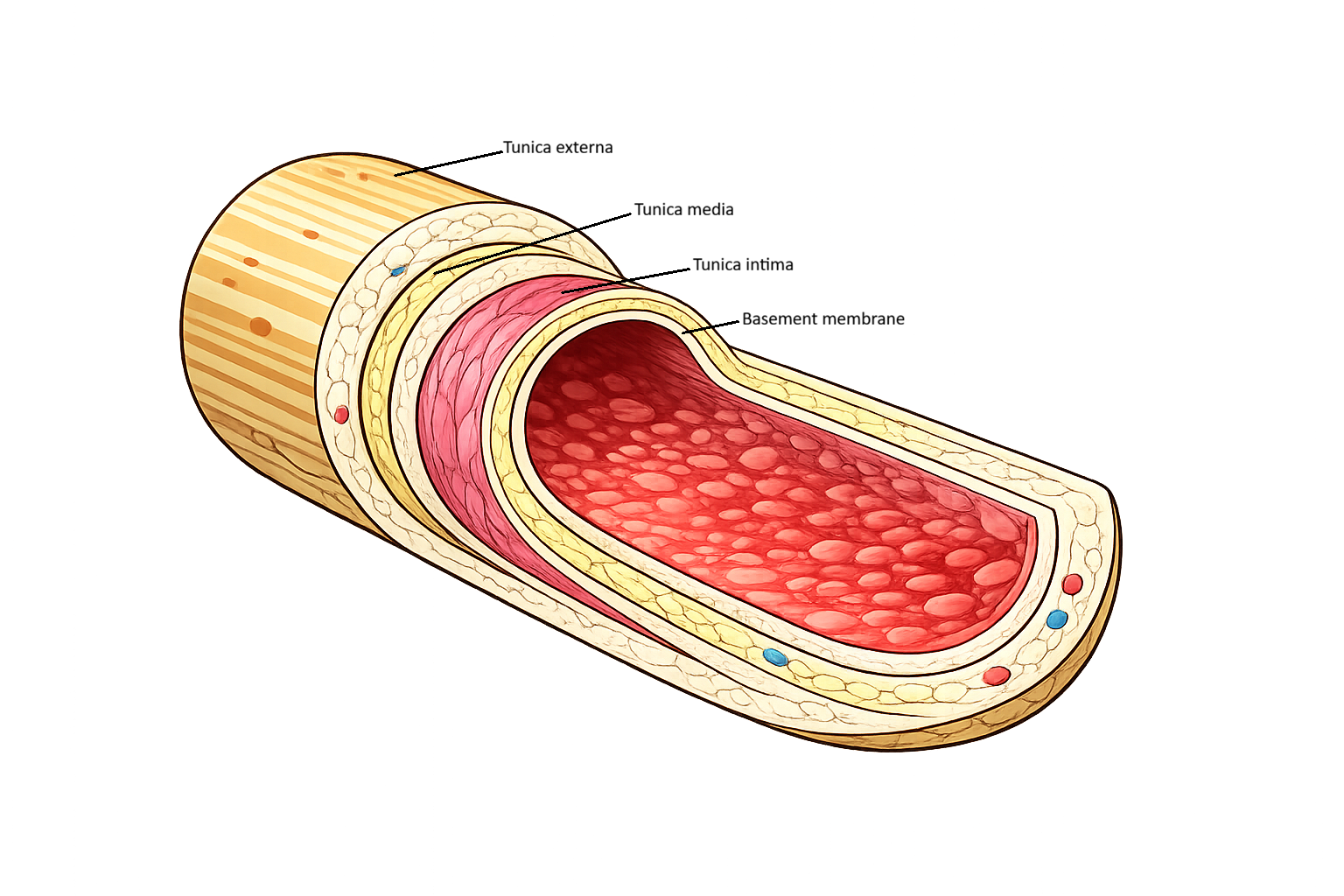
Image: the layers of a blood vessel.
Beyond the Basics
Structural Layers of Blood Vessels
All blood vessels share a common structural plan composed of three concentric layers, or tunics. These layers vary in thickness and composition depending on the vessel’s function, allowing the vascular system to withstand pressure, regulate flow, and support exchange.
The tunica intima is the innermost layer and consists of a single layer of endothelial cells resting on a thin basement membrane. This smooth, friction-reducing surface allows blood to flow efficiently and plays an active role in vascular homeostasis. Endothelial cells regulate permeability, secrete vasoactive substances, and help prevent inappropriate clot formation. In capillaries, the tunica intima is the only layer present, reflecting their primary role in exchange.
The tunica media lies external to the intima and is composed primarily of smooth muscle and elastic fibres. This layer is responsible for controlling vessel diameter and therefore resistance and blood pressure. The relative proportions of smooth muscle and elastin within the tunica media vary between vessel types, reflecting differences in pressure and regulatory function.
The tunica externa (or adventitia) is the outermost layer and consists mainly of connective tissue rich in collagen fibres. It provides structural support and anchors vessels to surrounding tissues. In larger vessels, the tunica externa also contains small blood vessels (vasa vasorum) and nerves that supply the vessel wall itself.
Layer Specialisation in Arteries
Arteries are exposed to high pressures generated by ventricular contraction, and their layered structure is due to this demand (structure often explains function in anatomy and physiology). Elastic arteries have a thick tunica media rich in elastin, allowing them to stretch during systole and recoil during diastole. This elastic behaviour dampens pressure fluctuations and maintains continuous blood flow between heartbeats.
Muscular arteries have a tunica media dominated by smooth muscle rather than elastic fibres. This structure enables precise regulation of vessel diameter, allowing blood flow to be directed toward or away from specific tissues. The tunica externa in arteries provides tensile strength to withstand the mechanical stress of pulsatile flow.
Arterioles and Resistance Control
Arterioles have a relatively thick tunica media compared to their lumen size, often consisting of just one or two layers of smooth muscle. This design makes them highly responsive to vasoconstrictive and vasodilatory signals. Because resistance is inversely related to vessel radius, small changes in arteriolar diameter have large effects on blood flow and pressure.
The tunica intima remains functionally important in arterioles, as endothelial signalling contributes to local control of tone. The tunica externa is thinner, reflecting the transition toward the microcirculation.
Capillary Structure and Exchange Efficiency
Capillaries consist almost entirely of the tunica intima, with endothelial cells and a basement membrane forming an extremely thin barrier. This minimal structure reduces diffusion distance and facilitates exchange of gases, nutrients, and waste products. Structural variations in capillary endothelium determine permeability, allowing each tissue to regulate what substances enter or leave the bloodstream.
Because capillaries lack a tunica media and externa, they cannot actively regulate diameter. Instead, blood flow through capillary beds is controlled upstream by arterioles.
Venous Layers and Capacitance Function
Veins operate under low pressure and therefore have thinner walls than arteries. Their tunica media contains less smooth muscle and elastin, while the tunica externa is often the thickest layer. This connective tissue support allows veins to accommodate large volumes of blood without generating high pressure.
Valves formed from folds of the tunica intima prevent retrograde flow, particularly in the limbs. The layered structure of veins supports their role as capacitance vessels, storing blood and returning it to the heart with assistance from external mechanisms rather than intrinsic pressure.
Structure Dictates Function
The organisation of the tunica intima, media, and externa underpins the functional diversity of the vascular system. From pressure buffering in elastic arteries to resistance control in arterioles, exchange in capillaries, and volume storage in veins, each vessel type reflects a precise balance between structure and role.
Understanding these layers provides a framework for appreciating how blood vessels respond to physiological demands and why different segments of the circulation behave so differently under stress.
Clinical Connections
Blood vessel disease reflects disruption of the specialised structure of arteries, veins, and capillaries. Arteries are designed to tolerate and regulate high pressure, but atherosclerosis progressively damages their elastic and muscular layers. Plaque buildup stiffens the vessel wall and narrows the lumen, increasing resistance and reducing downstream perfusion. When this occurs in different vascular beds it produces predictable patterns of disease:
Coronary arteries → angina, myocardial infarction
Cerebral arteries → stroke, transient ischaemic attacks
Peripheral arteries → claudication, cold limbs, non-healing ulcers
Because arterial blood delivers oxygen, reduced flow produces ischaemic pain, tissue pallor, cool skin, and delayed wound healing. These features reflect the failure of arteries to meet metabolic demand.
Venous disease arises from failure of the low-pressure return system. Veins depend on valves, skeletal muscle contraction, and respiratory pressure changes to move blood back to the heart. When valves fail or venous tone is impaired, blood pools in dependent limbs. This increases venous pressure and capillary filtration, leading to oedema, skin pigmentation, lipodermatosclerosis, and venous ulceration around the ankles.
In deep vein thrombosis (DVT), sluggish venous flow, endothelial injury, and hypercoagulability (Virchow’s triad) allow clot formation. Venous structure makes these clots particularly dangerous because they are not anchored to high-pressure walls. If dislodged, they travel through the venous system to the lungs, causing pulmonary embolism and acute right-sided heart strain.
Capillaries, though tiny, are often where major illness becomes visible. In sepsis, inflammatory damage to the endothelial barrier causes capillary leak, allowing plasma to escape into tissues. This reduces circulating volume, lowers blood pressure, and contributes to shock despite adequate heart function. The same mechanism explains why severe inflammation causes oedema and organ dysfunction.
Concept Check
Why do arteries have thicker walls than veins, and how does this relate to pressure differences?
How do venous valves and the muscle pump contribute to venous return?
What structural differences exist between continuous, fenestrated, and sinusoidal capillaries?
How does arteriole constriction influence systemic blood pressure?
What clinical signs differentiate arterial insufficiency from venous insufficiency?