The Cardiovascular System - Overview
The cardiovascular system is the body’s delivery service. Understanding this system is essential: it forms the foundation for interpreting pathophysiology, electrocardiograms (ECGs), and clinical conditions, as well as guiding assessments and interventions.
This article provides a foundational overview of the heart and vascular system, including blood flow through the heart and the pulmonary and systemic circuits. Later articles in this series will build on this knowledge, looking more closely at blood pressure regulation, the conduction system, and individual components of the cardiovascular system.
What You Need to know
The cardiovascular system is responsible for pumping blood around the body. It has three main components: a pump (the heart), vessels to carry the blood (arteries, veins and capillaries) and blood to transport gases, nutrients, hormones and waste products to and from every cell in the body. Therefore, it’s essentially a transport system. A complex, responsive and dynamic transport system.
The Heart
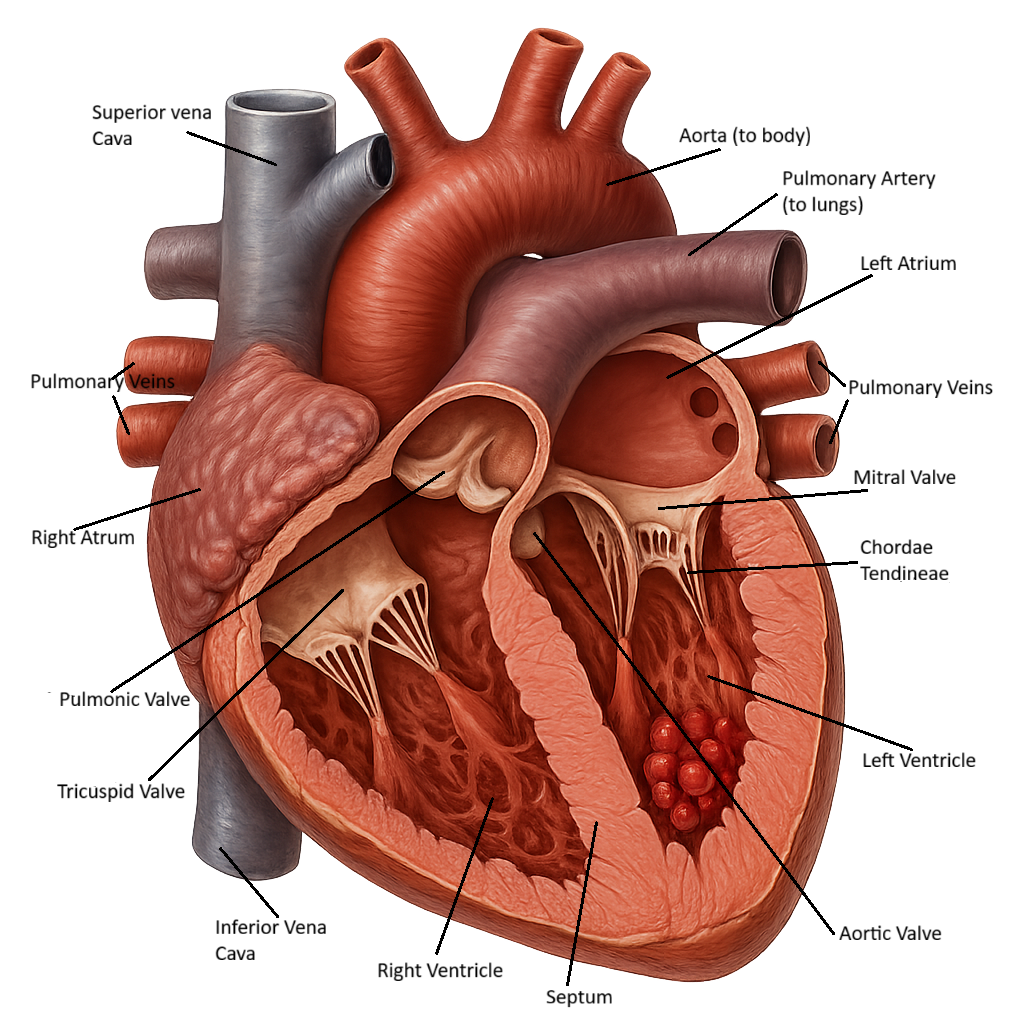
The heart is made up of four chambers – two atria, two ventricles, and four valves – the mitral, tricuspid, pulmonic and aortic valves. Blood moves through the chambers in a coordinated cycle. The valves prevent backflow of blood. Location of the valves:
Tricuspid valve – between the right atrium and right ventricle.
Pulmonic valve – between the right ventricle and pulmonary artery.
Mitral valve – between the left atrium and left ventricle.
Aortic valve – between the left ventricle and aorta.
The ventricles are not built the same. The left ventricle is heavily muscular because it needs to pump blood through the whole body at high pressure (normal systolic pressure in the aorta is 100–120 mmHg). The right ventricle, however, only pumps to the lungs. This circuit is much shorter and lower pressure, with normal systolic pressure in the pulmonary artery only 18–25 mmHg.
The Vascular System
The vascular components can be divided into two circuits: the pulmonary circuit and the systemic circuit. For the purposes of learning, a defined start and end point of both circuits is discussed here, but in reality, they form a continuous loop with no true beginning.
The Pulmonary Circuit
The pulmonary circuit starts at the right ventricle. The right ventricle pumps deoxygenated blood into the pulmonary trunk, which divides into the right and left pulmonary arteries (the only arteries that carry deoxygenated blood). The right pulmonary artery carries deoxygenated blood to the right lung, and the left pulmonary artery carries deoxygenated blood to the left lung. The right and left pulmonary arteries branch off into smaller arterioles and join the pulmonary capillary network. The capillaries are interconnected with alveolar in the lung. This is where gas exchange occurs. Oxygen diffuses from the alveolar into the blood and carbon dioxide diffuses from the blood into the alveolar. Essentially, the lungs exchange oxygen with carbon dioxide from the blood.
Now that gas exchange has occurred, blood will flow into the lung venules and veins and into the four pulmonary veins, two from each lung. The pulmonary veins carry blood into the left atrium. From the left atrium blood flows to the left ventricle.
The Systemic Circuit
The systemic circuit starts at the left ventricle, where blood which has been oxygenated by the pulmonary circuit is pumped into the aorta. From the aorta, major arteries branch off, progressively dividing into small arteries, arterioles and capillaries to deliver oxygen and nutrients to the cells of the body.
Blood Flow Through the Heart
Blood flows from the right atrium through the tricuspid valve and into the right ventricle. From the right ventricle, blood flows into the pulmonary circuit to be oxygenated. Oxygenated blood flows from the pulmonary veins to the left atrium, through the mitral valve and into the left ventricle to be pumped out to the body. The valve between the right ventricle and pulmonary artery is the pulmonic valve and the valve between the left ventricle and aorta is the aortic valve.
Beyond the Basics
The cardiovascular system functions to deliver oxygen and nutrients to tissues, remove metabolic waste, and maintain perfusion under changing physiological demands. Central to this system is the heart, which acts as a pressure-generating pump. To sustain this continuous activity, the heart requires its own dedicated blood supply, provided by the coronary circulation.
Integration with cardiac structure and function
The coronary circulation is structurally integrated into the heart and functionally linked to the cardiac cycle. Coronary arteries arise from the base of the ascending aorta, ensuring that oxygenated blood is delivered directly from the systemic circulation to the myocardium. Unlike most tissues, myocardial perfusion occurs predominantly during diastole, when ventricular relaxation reduces compression of the coronary vessels and allows blood to flow into the heart muscle.
This timing highlights the close relationship between coronary blood flow, ventricular pressure, and cardiac workload. Adequate diastolic pressure and sufficient diastolic duration are therefore essential for maintaining myocardial oxygen supply.
Coronary arterial supply
Two main coronary arteries supply the heart: the left and right coronary arteries. These vessels branch over the surface of the heart and penetrate the myocardium to deliver oxygenated blood to cardiac muscle cells. Major branches include the left anterior descending artery, the circumflex artery, and the right coronary artery, which together supply all regions of the atria and ventricles.
The distribution of coronary arteries reflects the functional demands of different regions of the heart, particularly the left ventricle, which generates the highest pressures and has the greatest metabolic requirements.
Venous drainage and circulation continuity
After oxygen extraction, deoxygenated blood is returned to the systemic circulation via the coronary venous system. Coronary veins collect blood from the myocardium and drain into the coronary sinus, which empties into the right atrium. This completes the coronary circuit and ensures continuous clearance of metabolic by-products from cardiac tissue.
The close coupling of coronary arterial supply and venous drainage allows efficient regulation of myocardial perfusion within the overall circulatory system.
Relationship to systemic circulation and regulation
The coronary circulation operates as part of the systemic circulation but possesses specialised regulatory mechanisms. Because myocardial oxygen extraction is already high at rest, increases in cardiac demand are met primarily by increasing coronary blood flow rather than by extracting more oxygen from the blood. This reliance on flow highlights the importance of intact coronary vessels and appropriate vascular regulation.
Neural, metabolic, and local endothelial factors all contribute to adjusting coronary vessel tone in response to changes in cardiac workload, ensuring that supply matches demand under normal conditions.
Clinical relevance within the cardiovascular system
Disruption of coronary blood flow compromises the heart’s ability to function as an effective pump, with consequences for the entire cardiovascular system. Ischemia reduces myocardial contractility and can impair electrical conduction, while infarction leads to permanent loss of functional muscle tissue.
Because the left anterior descending artery supplies a large proportion of the left ventricle, obstruction in this vessel has particularly serious implications for cardiac output and systemic perfusion. Understanding coronary circulation at a systems level provides essential context for later discussions of ischemic heart disease, heart failure, and cardiovascular regulation.
Clinical Connections
Thinking of cardiovascular disease as problems with the pump, the pipes, or the circulation provides a helpful framework for bedside assessment and escalation.
When the pump fails, as in heart failure, cardiomyopathy, or severe valve disease, cardiac output falls. This leads to poor organ perfusion and fluid backup. Clinically this produces breathlessness, pulmonary crackles, oedema, fatigue, hypotension, and reduced urine output. Rising respiratory rate, falling oxygen saturation, and increasing weight from fluid retention long before overt decompensation occurs are often manifestations of heart failure.
When the pipes (blood vessels) are blocked, tissues downstream become ischaemic. In coronary artery disease this can present as chest pain, ECG changes, and troponin elevation. In peripheral arterial disease it causes claudication, cold limbs, reduced pulses, and non-healing wounds. In the brain it produces stroke or transient neurological deficits. Early recognition of pain patterns, pulse changes, and skin temperature is crucial to prevent permanent tissue injury.
When the circulation is disrupted, blood flow may be inadequate or misdirected despite a functioning heart. Pulmonary embolism prevents blood from reaching the lungs for oxygenation. Sepsis causes vasodilation and capillary leak, leading to shock. Severe hypertension increases resistance, while haemorrhage reduces circulating volume. These conditions often present with tachycardia, altered blood pressure, mottled skin, confusion, and reduced urine output.
Across all three categories, close monitoring of clinical manifestations can guide treatment. In a clinical setting, the following should be routinely monitored:
heart rate, blood pressure, respiratory rate, and oxygen saturation
skin colour, temperature, and capillary refill
mental state and urine output
Small changes in these parameters can indicate a shift in cardiovascular function. Early recognition allows timely intervention before organ damage occurs.
Concept Check
How would left-sided heart failure change blood flow through the lungs and affect oxygenation?
How would damage to a heart valve (for example, mitral or aortic) alter pressure, volume, and flow through the heart chambers?
How would high blood pressure affect the heart and systemic circuit over time?
How would blockage of the coronary arteries affect heart function?
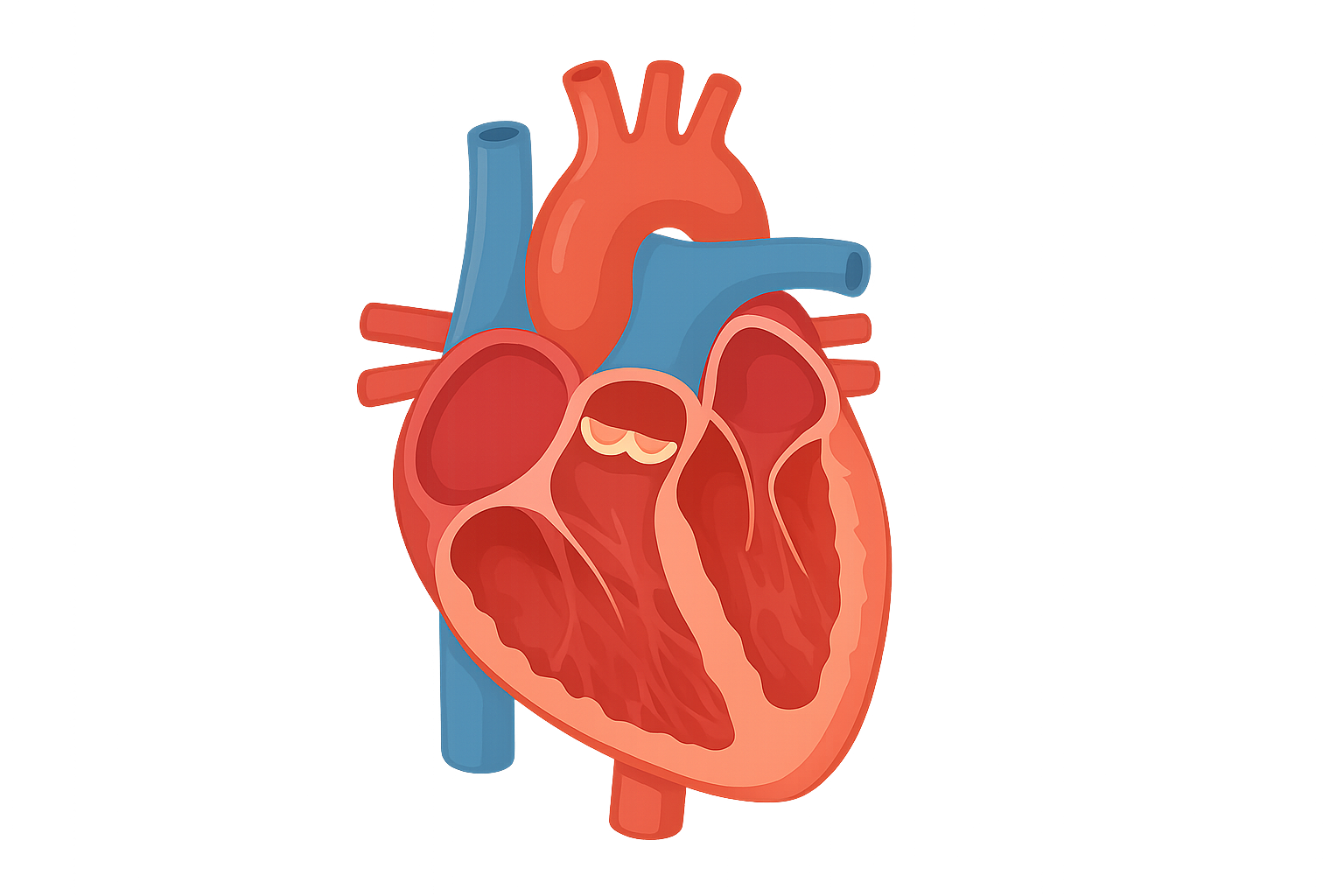
Label the picture of the heart below with the chambers, valves, major blood vessels and direction of blood flow.