The Cardiac Cycle: Systole, Diastole & the Dynamics of a Heartbeat
The cardiac cycle is the sequence of mechanical events that occurs with every heartbeat. It includes periods of contraction and relaxation that allow the heart to fill with blood, pump it forward, and maintain continuous circulation throughout the body. Although often described simply as systole and diastole, the cardiac cycle is a complex interplay of pressure changes, valve movements, and chamber dynamics. Understanding these phases is essential for interpreting heart sounds, ECG rhythms, blood pressure readings, and clinical manifestations of cardiac dysfunction. For nursing students, mastery of the cardiac cycle provides a foundation for almost all aspects of cardiovascular assessment.
What You Need to Know
The cardiac cycle is the repeating sequence of mechanical events that allows the heart to fill with blood and then pump it forward to the lungs and the rest of the body. Each heartbeat consists of two coordinated phases: diastole, when the ventricles relax and fill, and systole, when the ventricles contract and eject blood. Both phases are equally important: without adequate filling during diastole, there is insufficient blood to eject during systole, and cardiac output falls.
The cycle begins with ventricular diastole. As the ventricles relax, pressure inside them drops below the pressure in the atria. This pressure gradient causes the atrioventricular (AV) valves — the mitral valve on the left and the tricuspid valve on the right — to open. Blood flows passively from the atria into the ventricles, filling them smoothly. This passive phase provides the majority of ventricular filling.
Near the end of diastole, the atria contract in a phase known as the atrial kick, which pushes the remaining blood into the ventricles and ensures optimal end-diastolic volume, particularly when the heart rate is slow or the ventricles are stiff.
At this point in the cycle:
The ventricles are maximally filled
The AV valves are open
The semilunar valves are closed
Ventricular systole begins when the ventricles start to contract. Rising ventricular pressure forces the AV valves to close, preventing blood from flowing back into the atria and producing the first heart sound (S1). For a brief moment all valves are closed while pressure continues to rise. When ventricular pressure exceeds the pressure in the pulmonary artery and aorta, the semilunar valves open and blood is ejected into the circulation.
As contraction ends, ventricular pressure falls. When it drops below the pressure in the great arteries, the semilunar valves snap shut, producing the second heart sound (S2). The ventricles then relax, pressure falls further, the AV valves reopen, and the next cycle of filling begins. This precisely timed sequence ensures efficient, one-way movement of blood through the heart with every heartbeat.
Beyond the Basics
Phases of Ventricular Filling
Diastole is an active, energy-dependent process rather than a purely passive resting phase. Ventricular relaxation begins immediately after systole, as calcium is re-sequestered (taken back into storage, so the heart muscle can relax) into the sarcoplasmic reticulum, allowing myocardial fibres to lengthen. As ventricular pressure falls below atrial pressure, the AV valves open and rapid passive filling begins. Blood flows down a pressure gradient from the atria into the ventricles, accounting for the majority of ventricular filling under normal conditions.
As filling continues, the pressure gradient between the atria and ventricles narrows and ventricular filling slows. This mid-diastolic phase, often termed diastasis, represents a period of relative equilibrium. Toward the end of diastole, atrial contraction provides the final contribution to ventricular filling. This atrial kick is particularly important when ventricular compliance is reduced or when heart rate is increased, as it helps optimise end-diastolic volume and stroke volume.
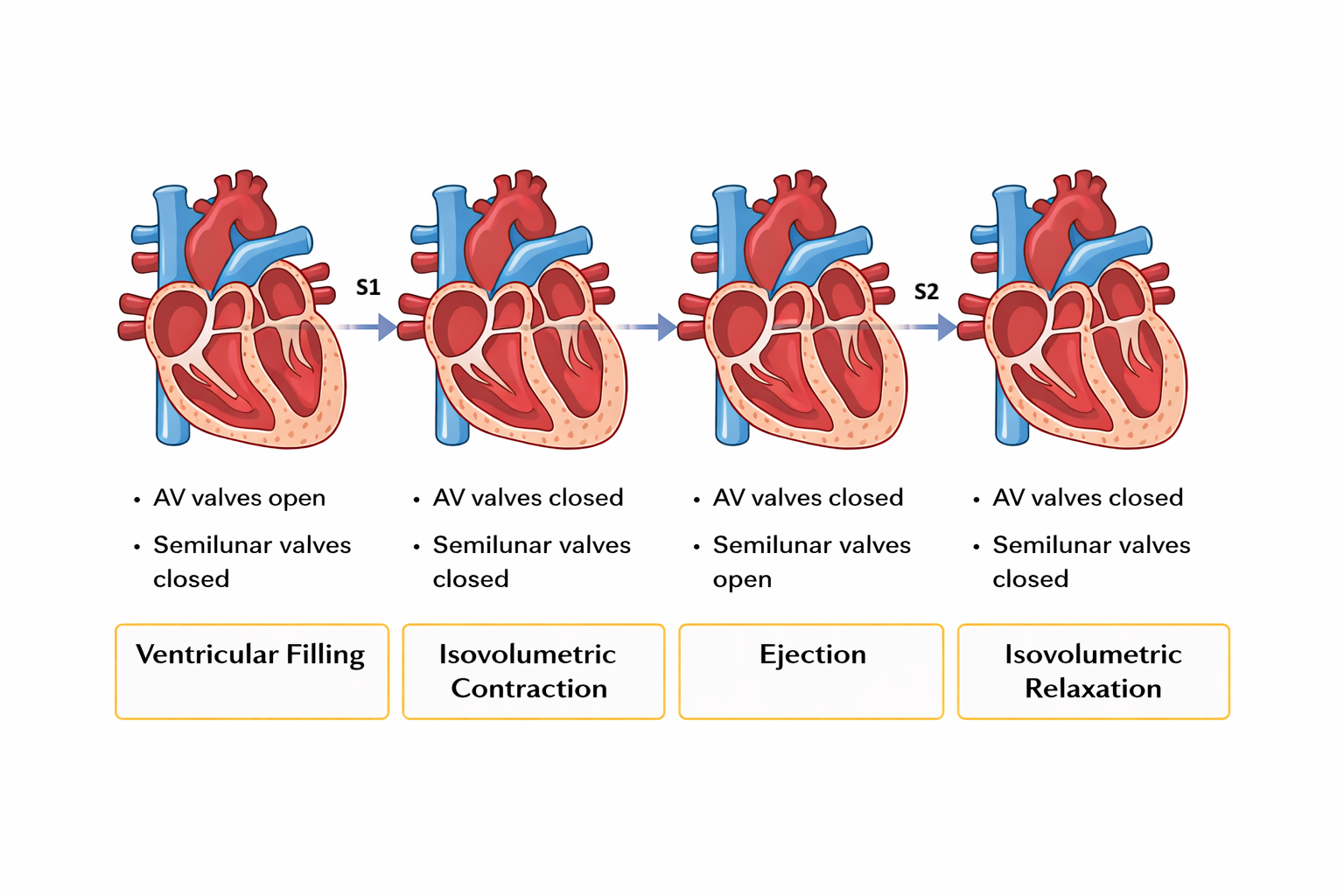
Image: Cardiac cycle phases. Ventricular filling → isovolumetric contraction (S1) → ejection → isovolumetric relaxation (S2), with valve opening and closing coordinating blood flow through the heart.
Isovolumetric Contraction and the Onset of Systole
Systole begins with ventricular depolarisation, which triggers coordinated myocardial contraction. As ventricular pressure rises, it rapidly exceeds atrial pressure, forcing the AV valves to close. Because all valves are closed at this moment, ventricular volume remains constant despite increasing pressure, a phase known as isovolumetric contraction. The sudden closure of the AV valves generates vibrations within the cardiac structures and surrounding blood, producing the first heart sound (S1).
During this phase, pressure builds rapidly within the ventricles without any blood being ejected. This pressure generation is essential to overcome the resistance of the systemic and pulmonary circulations. The duration of isovolumetric contraction is brief but critical, setting the conditions for effective ventricular ejection.
Ventricular Ejection and Pressure Dynamics
Once ventricular pressure exceeds the pressure within the aorta and pulmonary artery, the semilunar valves open and ventricular ejection begins. Early systole is characterised by rapid ejection as blood is forcefully expelled into the great arteries. Ventricular pressure continues to rise during this phase, reaching its peak in mid-systole as myocardial contraction is strongest.
As systole progresses, ventricular contraction weakens and the rate of ejection slows. Although blood continues to leave the ventricles, pressure begins to fall as muscle fibres shorten and tension decreases. This late ejection phase marks the transition toward ventricular relaxation, even while the semilunar valves remain open.
Isovolumetric Relaxation and Valve Closure
Systole ends as ventricular pressure falls below arterial pressure. This reversal of the pressure gradient causes the semilunar valves to close, preventing backflow of blood into the ventricles. The closure of these valves generates the second heart sound (S2), which is typically sharper and shorter than S1 due to the higher pressures involved.
Following semilunar valve closure, the ventricles enter isovolumetric relaxation. During this phase, all valves are closed and ventricular volume remains unchanged while pressure drops rapidly. This pressure decline is driven by myocardial relaxation and is essential for the subsequent reopening of the AV valves and the start of the next diastolic filling phase.
Integration of Electrical and Mechanical Events
The cardiac cycle reflects tight coupling between electrical activity and mechanical function. Electrical depolarisation precedes contraction, while repolarisation precedes relaxation. Any disruption to this sequence, such as conduction delays or arrhythmias, can impair the timing of valve movements and reduce cardiac efficiency.
Understanding the cardiac cycle as a continuous, coordinated sequence rather than isolated events helps explain how changes in heart rate, rhythm, or ventricular compliance alter cardiac performance. Each phase prepares the heart for the next, ensuring efficient filling, ejection, and maintenance of forward blood flow with every beat.
Clinical Connections
The cardiac cycle provides a framework for interpreting heart sounds, blood pressure, and symptoms of cardiovascular disease. Abnormalities in the timing or mechanics of diastole and systole often reveal underlying pathology. A loud or abnormally split S2 may indicate pulmonary hypertension, delayed right ventricular emptying, or aortic valve disease. An S3 heart sound results from rapid ventricular filling into an already overloaded ventricle and is a classic finding in heart failure. An S4 occurs when the atria contract against a stiff, non-compliant ventricle and is commonly associated with long-standing hypertension, left ventricular hypertrophy, or ischaemic heart disease.
Different patterns of dysfunction relate to specific phases of the cardiac cycle:
Systolic dysfunction reduces stroke volume and ejection fraction, leading to hypotension, fatigue, and poor tissue perfusion
Diastolic dysfunction impairs ventricular filling, causing pulmonary congestion and exertional dyspnoea even when systolic function appears preserved
Valve disease alters pressure relationships between chambers, producing characteristic murmurs and abnormal heart sounds
The cardiac cycle also explains the effects of many cardiovascular medications. Beta-blockers slow the heart rate, prolonging diastole and improving ventricular filling and coronary perfusion. Vasodilators reduce afterload, allowing the ventricles to eject blood more easily during systole. Diuretics lower preload by reducing circulating volume, decreasing ventricular stretch and relieving pulmonary congestion.
Concept Check
What mechanical events produce S1 and S2?
Why does tachycardia reduce ventricular filling?
What is the significance of the atrial kick?
How do isovolumetric phases contribute to valve timing?
What might an S3 or S4 sound indicate clinically?