Structure of the Skin Layers: Epidermis, Dermis, and Hypodermis
The skin is a dynamic, multilayered organ that forms the body’s primary physical barrier against the external environment. Beyond its obvious protective role, it regulates temperature, prevents dehydration, supports sensory perception, participates in immune defence and interacts with the endocrine system through vitamin D synthesis. Each of its three major layers, the epidermis, dermis and hypodermis, contains specialised cellular and structural components that contribute uniquely to the skin’s resilience and function. Understanding these layers is essential for interpreting wound depth, dermatological conditions, thermoregulation and systemic diseases that manifest in the skin.
What You Need to Know
The skin is organised into three structurally and functionally distinct layers: the epidermis, dermis and hypodermis. Each layer has specialised roles, but none functions in isolation. Together, they form a coordinated system that provides protection, sensation, immune defence, temperature regulation and metabolic support. Damage or dysfunction in one layer inevitably affects the others, which is why skin injury often has wider physiological consequences.
The epidermis is the outermost layer and acts as the primary protective barrier. It is composed of stratified squamous keratinised epithelial cells that undergo continuous renewal. Basal keratinocytes divide, differentiate and migrate toward the surface, eventually forming the stratum corneum. This process maintains barrier integrity while allowing constant turnover. The epidermis also contains specialised cells, including melanocytes, Langerhans cells and Merkel cells, linking barrier function with pigmentation, immunity and sensation.
The dermis lies beneath the epidermis and provides most of the skin’s mechanical strength and elasticity. It is composed of dense connective tissue rich in collagen, elastin and ground substance. This layer houses blood vessels, lymphatics, nerves, hair follicles, sweat glands and sebaceous glands. Through its vascular network, the dermis supports nutrient delivery, thermoregulation and immune cell trafficking. Its structural proteins allow the skin to stretch, recoil and resist mechanical stress without tearing.
The hypodermis, also known as the subcutaneous layer, anchors the skin to underlying muscle and bone. It is composed primarily of adipose tissue and loose connective tissue, providing cushioning, insulation and energy storage. This layer also serves as a conduit for larger blood vessels and nerves supplying the skin and deeper structures.
Key functional contributions of each layer include:
Epidermis: barrier protection, prevention of water loss, immune surveillance and pigmentation
Dermis: tensile strength, elasticity, sensation, thermoregulation and vascular support
Hypodermis: insulation, shock absorption, energy storage and structural anchoring
Although described as separate layers, the epidermis, dermis and hypodermis operate as an integrated unit. Immune signals initiated in the epidermis influence dermal blood flow and inflammatory responses. Dermal vascular changes affect epidermal nutrition and repair. Hypodermal insulation alters heat exchange at the skin surface. Understanding this layered organisation is essential for interpreting wound depth, disease processes and the systemic impact of skin injury.
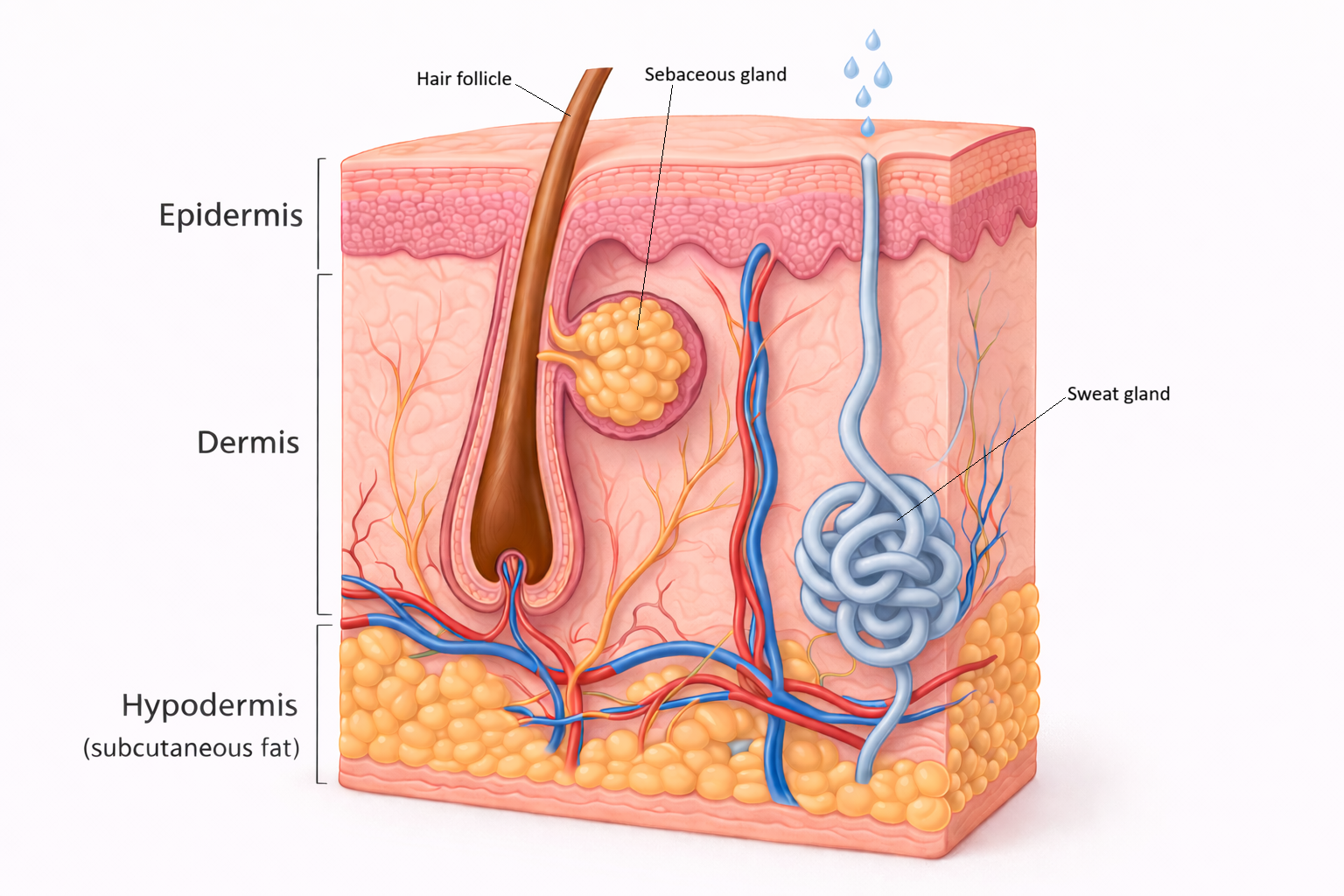
Image: Layers of the skin/
Beyond the Basics
The Epidermis
The epidermis is a highly specialised, self-renewing epithelial layer composed predominantly of keratinocytes derived from stem cells in the stratum basale. These basal cells undergo continuous mitosis, supplying new cells that migrate upward while progressively differentiating. This orderly movement ensures that the epidermis maintains barrier integrity despite constant exposure to mechanical stress, microorganisms and environmental chemicals.
As keratinocytes enter the stratum spinosum, they develop extensive desmosomal connections with neighbouring cells. These junctions provide mechanical cohesion and distribute shear forces across the epidermis, which explains the characteristic spiny appearance seen histologically. In the stratum granulosum, keratinocytes undergo a major biochemical transition. Keratohyalin granules rich in profilaggrin accumulate, supporting keratin aggregation, while lamellar bodies release lipids into the extracellular space. These lipids organise into lamellar sheets that form the hydrophobic barrier responsible for limiting transepidermal water loss.
In thick skin, such as the palms and soles, the stratum lucidum provides additional mechanical protection in areas subjected to high friction and pressure. The outermost stratum corneum consists of flattened, anucleate corneocytes embedded in a lipid matrix. Although these cells are dead, they are functionally active as a barrier, being continuously shed and replaced through tightly regulated desquamation. This dynamic turnover allows the epidermis to remain protective while adapting to injury and environmental change.
Several specialised cell types enhance epidermal function. Melanocytes in the basal layer synthesise melanin and transfer it to surrounding keratinocytes, reducing ultraviolet-induced DNA damage. Langerhans cells act as immune sentinels, sampling antigens and initiating adaptive immune responses when threats are detected. Merkel cells form connections with sensory nerve endings, contributing to fine touch perception in areas requiring high tactile resolution.
The Dermis
The dermis forms the structural and functional core of the skin and is substantially thicker than the epidermis. Its papillary layer consists of loose connective tissue with fine collagen and elastic fibres, along with capillary loops that supply nutrients and oxygen to the avascular epidermis. The interdigitation of dermal papillae with epidermal ridges strengthens attachment between layers and increases surface area, contributing to mechanical stability and the formation of fingerprints.
Beneath this lies the reticular layer, composed of dense irregular connective tissue. Thick collagen bundles arranged in multiple orientations allow the skin to resist stretching, compression and shear from different directions. Elastin fibres woven through this matrix provide recoil, enabling the skin to return to its original shape after deformation. Ageing, ultraviolet exposure and disease alter this collagen–elastin balance, leading to reduced strength and elasticity.
The dermis houses a rich array of sensory receptors that detect touch, pressure, vibration, pain and temperature. It also contains an extensive vascular network capable of rapid vasodilation and vasoconstriction, making the dermis central to thermoregulation. Through these vascular responses, the skin can either dissipate heat or conserve it, linking structural anatomy with physiological regulation.
Skin appendages originate within the dermis. Hair follicles, sebaceous glands and sweat glands contribute to lubrication, temperature control and chemical signalling. Importantly, these structures also provide reservoirs of epithelial cells that support re-epithelialisation following superficial injury, enhancing the skin’s capacity for repair.
The Hypodermis
The hypodermis, or subcutaneous tissue, lies beneath the dermis and is composed mainly of adipocytes arranged in lobules separated by fibrous connective tissue septa. Its thickness varies according to anatomical location, age, sex and nutritional status. Functionally, this layer serves as a thermal insulator, slowing heat loss from the body, and as a shock absorber that protects deeper tissues from mechanical trauma.
Adipose tissue within the hypodermis also acts as an energy reserve, storing triglycerides that can be mobilised during periods of increased metabolic demand. In addition, the hypodermis provides a low-friction interface that allows the skin to move over underlying muscles and bones without tearing.
Because it contains larger blood vessels and nerves en route to the skin and deeper structures, the hypodermis is clinically significant. Its vascularity makes it a common site for subcutaneous medication administration, where slower absorption is often desirable.
Integration Between Layers
Although the skin is described in layers, its function depends on close integration between the epidermis, dermis and hypodermis. The epidermis relies on the dermis for nutrition, immune support and repair mechanisms, while the dermis depends on an intact epidermal barrier to prevent infection and excessive fluid loss. Injury to one layer inevitably affects the others.
The hypodermis contributes mechanical flexibility, cushioning and thermal buffering, allowing the skin to withstand environmental stress while maintaining internal stability. Together, these layers coordinate responses to injury, temperature change and microbial exposure through interconnected vascular, immune and cellular pathways. This integration is fundamental to the skin’s role as a resilient, adaptive organ rather than a simple protective covering.
Clinical Connections
Understanding the layered structure of the skin provides a practical framework for interpreting the severity, consequences and healing potential of injury and disease. Because each layer contributes differently to protection, sensation, vascular supply and regeneration, the depth of tissue involvement directly determines clinical risk and management.
Burn injury is a clear example of layer-dependent pathology. Superficial burns are limited to the epidermis and typically present with erythema and pain but heal without scarring because dermal structures remain intact. Partial-thickness burns extend into the dermis, damaging blood vessels, nerve endings and skin appendages, which increases pain, fluid loss and infection risk. Full-thickness burns destroy both the epidermis and dermis, eliminating local regenerative capacity and necessitating surgical intervention such as skin grafting.
Layer-specific involvement is also central to many chronic conditions:
Epidermal disorders such as eczema and psoriasis involve abnormal keratinocyte turnover, immune dysregulation and impaired barrier function
Dermal degeneration, as seen in ageing and photo-damage, reflects collagen fragmentation and elastin loss, leading to thinning, wrinkling and reduced mechanical resilience
Vascular compromise within the dermis and hypodermis underlies pressure injuries, where prolonged compression impairs perfusion and causes tissue ischaemia
Deep tissue injury involving the hypodermis may occur before visible epidermal breakdown, particularly in immobile or critically ill patients
Pressure injuries highlight the importance of the dermis and hypodermis in tissue viability. Sustained pressure, friction and shear reduce capillary blood flow, leading to hypoxia, cellular death and eventual skin breakdown. Because early damage may occur below the surface, routine inspection and risk assessment are essential for prevention.
Accurately identifying which skin layers are affected allows clinicians to anticipate healing potential, infection risk and the need for intervention. This layered understanding informs wound classification, dressing selection, escalation of care and patient education, reinforcing why anatomical knowledge is essential for safe and effective clinical decision-making.
Concept Check
How do keratinocyte differentiation and lipid secretion contribute to the epidermal barrier?
Why does the dermis provide structural strength while the epidermis provides protection?
How does the hypodermis support both mechanical protection and metabolic function?
Why do deep partial-thickness and full-thickness burns impair wound healing?
How do melanocytes and Langerhans cells enhance the skin’s protective functions?