Nail Anatomy: Structure, Growth and Functional Significance
Nails are highly specialised epidermal structures composed of densely packed, keratinised cells. Although anatomically simple at first glance, they serve important protective, sensory and functional roles. Nails enhance the precision of fingertip movements, provide counter-pressure to improve tactile sensitivity, and shield the distal phalanges from trauma. Their structure reflects a continuous interaction between the nail matrix, nail bed, surrounding folds and underlying vascular supply. Knowledge of nail anatomy can assist in interpreting clinical signs, diagnosing systemic disease and recognising pathological changes such as fungal infections, trauma patterns and nutritional deficiencies.
What You Need to Know
The nail unit is a specialised keratinised structure that protects the distal digits and enhances fine motor function and sensation. Although the nail plate itself is composed of hard, dead keratin, nail growth and integrity depend on a complex underlying apparatus that includes the nail matrix, nail bed and surrounding protective tissues. Continuous interaction between these components allows nails to grow steadily while remaining firmly attached to the fingertip.
Key anatomical and functional components of the nail include:
The nail plate, a hard, translucent structure that provides protection and counter-pressure for fingertip sensation
The nail matrix, a highly proliferative region responsible for producing the nail plate
The nail bed, a vascular tissue that supports adhesion of the nail plate and contributes to its pink appearance
Protective structures such as the proximal and lateral nail folds, cuticle and hyponychium, which seal the nail unit and prevent microbial entry
Nails grow continuously from the matrix, with fingernails typically growing faster than toenails. Growth rate is influenced by age, circulation, nutrition, hormonal status and systemic health. Because the nail plate records changes as it grows, alterations in colour, thickness, shape or surface can reflect local trauma or underlying systemic disease. Nails therefore serve not only as protective tools but also as visible indicators of physiological and pathological processes within the body.
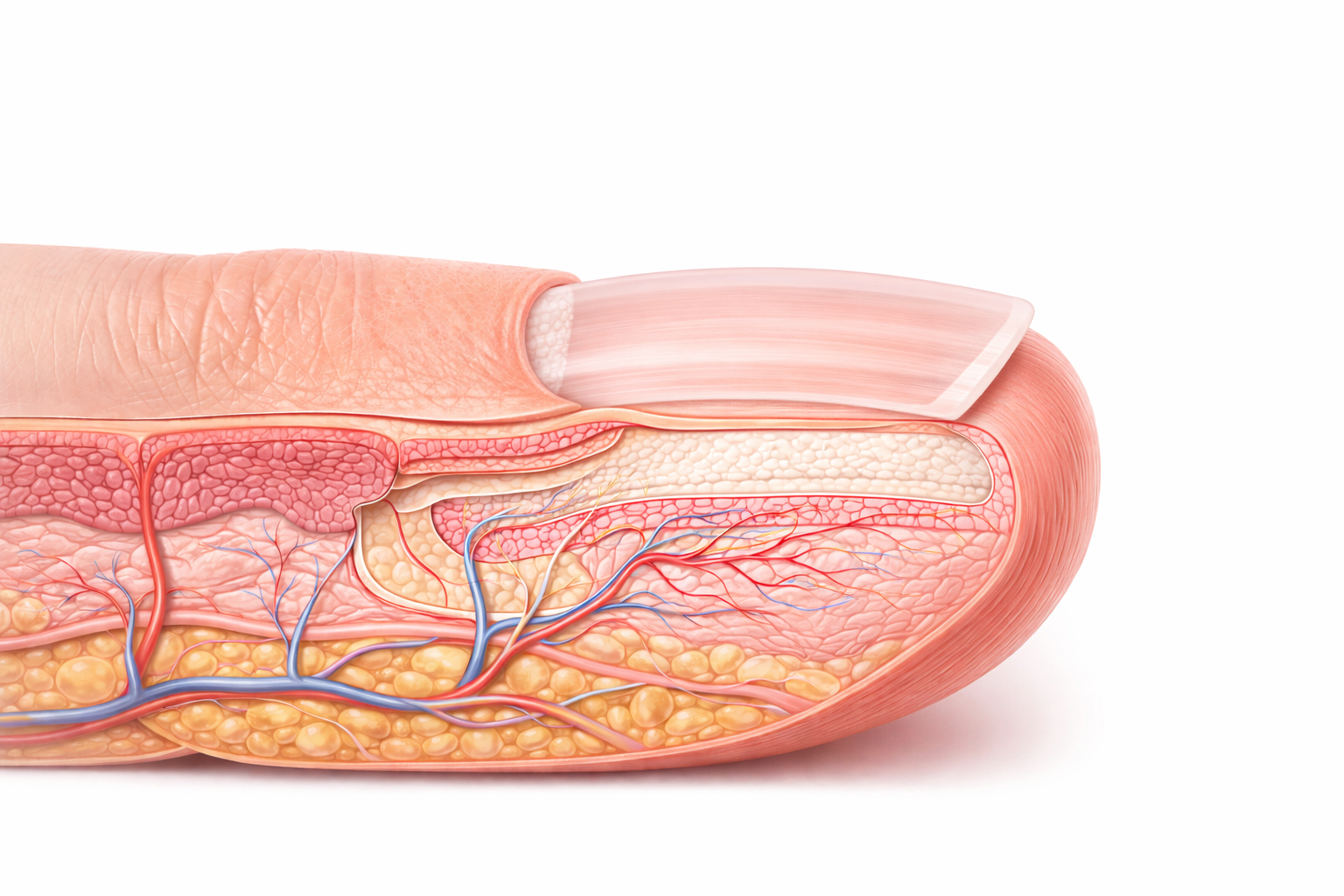
Image: The nail plate is produced by the nail matrix, a specialised region of proliferating cells located beneath the proximal nail fold. As these cells keratinise, they form the hard nail plate, which slides distally over the vascular nail bed, while surrounding structures such as the cuticle and hyponychium act as protective barriers.
Beyond the Basics
Nail plate structure and composition
The nail plate is a flattened, translucent structure composed of densely compacted keratinocytes filled with hard keratin. This keratin is richer in disulphide bonds than epidermal or hair keratin, giving the nail its characteristic rigidity and resistance to mechanical stress. The tightly bound cells form a smooth, continuous surface that protects the distal digit while still allowing precision and fine motor control.
Because the nail plate is translucent, it permits visualisation of the vascular nail bed beneath. Changes in thickness, surface smoothness or colour often reflect alterations in matrix activity, keratin organisation or underlying perfusion, making the nail plate a sensitive indicator of both local and systemic change.
Nail matrix as the growth centre
The nail matrix is the proliferative engine of the nail unit. Located beneath the proximal nail fold, it contains rapidly dividing keratinocytes that continuously generate the nail plate. As these cells differentiate, they flatten and harden, forming successive layers that are pushed distally as new nail is produced.
The lunula represents the distal portion of the matrix and appears pale because the thickened, partially keratinised nail plate obscures the underlying vasculature. Injury or disease affecting the matrix can have lasting consequences, as damage to this region disrupts keratinocyte proliferation and differentiation. Depending on severity and duration, this may result in permanent ridging, thinning, thickening or distortion of the nail plate.
Nail bed and mechanisms of adherence
The nail bed is a specialised epithelial layer firmly attached to the underlying dermis. Unlike surface epidermis, the nail bed epithelium is arranged in longitudinal ridges that interlock with corresponding grooves on the underside of the nail plate. This structural arrangement secures the plate while still allowing it to slide forward as growth occurs.
Beneath the nail bed lies a dense capillary network that contributes to the pink appearance of healthy nails. Alterations in blood flow, oxygenation or pigmentation are readily visible through the translucent plate, which is why nails are commonly assessed for signs of circulatory, respiratory or systemic disease.
Protective nail folds, cuticle and hyponychium
The proximal and lateral nail folds surround and protect the emerging nail plate. The cuticle, or eponychium, forms a tight seal between the proximal fold and the nail plate, preventing microorganisms, moisture and irritants from entering the matrix region. Disruption of this seal, whether through trauma, aggressive grooming or inflammation, increases susceptibility to infection.
At the distal end, the hyponychium forms a second protective barrier beneath the free edge of the nail. Its thickened keratinised tissue prevents microbial entry from the fingertip side and provides mechanical support during gripping and fine manipulation. Together, these structures maintain the integrity of the nail apparatus.
Growth patterns and influencing factors
Nails grow continuously, with fingernails typically growing faster than toenails. Growth rate is influenced by age, hormonal status, circulation, temperature, nutritional status and overall health. Acute illness, trauma or systemic stress can temporarily interrupt matrix activity, producing transverse depressions known as Beau’s lines.
Because fingernails grow at an average rate of 2–3 millimetres per month, visible changes in the nail plate reflect past events rather than immediate pathology. This slow growth allows nails to act as a chronological record of physiological stress, nutritional deficiency or disease.
Functional significance of nails
Nails play an important mechanical and sensory role. By providing a rigid backing to the soft tissue of the fingertip, they enhance precision grip and fine motor control. This counter-pressure improves tactile discrimination by increasing activation of mechanoreceptors in the digital pulp.
Toenails protect the distal toes from repetitive mechanical stress during walking and weight-bearing. Across all digits, nails function as protective shields, sensory amplifiers and visible indicators of internal health, integrating structural, neurological and vascular roles within a compact anatomical unit.
Clinical Connections
Changes in nail appearance often reflect disturbances in systemic physiology, local circulation or the integrity of the nail apparatus itself. Because nails grow slowly and are richly supplied by vascular and connective tissue structures, abnormalities may reveal chronic or past pathology rather than acute illness.
In clinical assessment, nail abnormalities most commonly signal:
Systemic disease affecting oxygenation, circulation or nutrition
Inflammatory or infectious conditions involving the nail unit
Local trauma or matrix damage
Clubbing reflects chronic hypoxia and altered connective tissue growth within the distal digits, most often associated with pulmonary or cardiovascular disease. Spoon-shaped nails, or koilonychia, are classically linked to iron deficiency and reflect impaired keratinisation and structural weakness. Splinter haemorrhages arise from capillary damage within the nail bed and may be traumatic in origin or associated with systemic conditions such as infective endocarditis.
Local nail disease is also common. Onychomycosis produces thickened, discoloured and brittle nails due to fungal invasion of the plate and bed, while psoriasis may cause pitting, onycholysis or the characteristic oil-drop discoloration resulting from inflammatory changes beneath the nail plate. Trauma to the nail unit can disrupt the matrix or bed, leading to subungual haematomas, ridging or permanent growth abnormalities depending on the extent of injury.
Concept Check
How does the nail matrix contribute to the continuous growth of the nail plate?
Why is the nail plate translucent, and what determines its colour?
How do the nail folds and cuticle protect the underlying matrix?
Why do injuries to the nail bed or matrix leave long-lasting visible marks?
What clinical conditions can alter the thickness or contour of the nail plate?