TONSILS: STRUCTURE & FUNCTION
Tonsils are specialised lymphoid structures located at the entrance of the respiratory and digestive tracts. Their strategic position allows them to detect airborne and ingested pathogens quickly, making them essential components of the body’s first line of immune defence. Unlike lymph nodes, which filter lymph, tonsils directly sample material entering the body, initiating early immune responses through antigen capture and lymphocyte activation.
What You Need to Know
Tonsils are organised collections of lymphoid tissue positioned at the entrance of the respiratory and gastrointestinal tracts, where exposure to inhaled and ingested antigens is constant. Together, the palatine, lingual, and pharyngeal tonsils form Waldeyer’s ring, creating an immunological barrier at the oropharynx and nasopharynx. Their location allows early sampling of microbes before pathogens reach deeper tissues.
Several structural features support this surveillance role:
Lymphoid follicles with germinal centres, where B cells proliferate and undergo differentiation
Overlying epithelium that directly interfaces with the external environment
Deep epithelial crypts that increase surface area and trap antigens
Close proximity of antigen-presenting cells, T cells, and B cells to enable rapid activation
Antigens captured within tonsillar crypts are processed by dendritic cells and presented to lymphocytes within the underlying lymphoid tissue. This leads to activation of T cells and production of antibodies, particularly IgA, which supports mucosal defence. Because this process occurs locally and continuously, tonsils contribute to rapid immune responses against common respiratory and oral pathogens.
Tonsillar immune activity is especially important in early life. Repeated antigen exposure during childhood supports maturation of adaptive immune responses and development of immunological memory. Through this constant interaction with environmental antigens, tonsils help shape immune responsiveness while maintaining tolerance to non-threatening substances encountered at mucosal surfaces.
Their surface is covered in epithelium featuring deep crypts that dramatically increase surface area, allowing tonsils to trap bacteria, viruses and food particles. This exposure stimulates rapid immune activation, including antibody production and T cell responses. Because tonsils sit directly at mucosal interfaces, they play a critical role in developing early-life immunity, shaping the immune system’s response to common pathogens encountered throughout childhood.
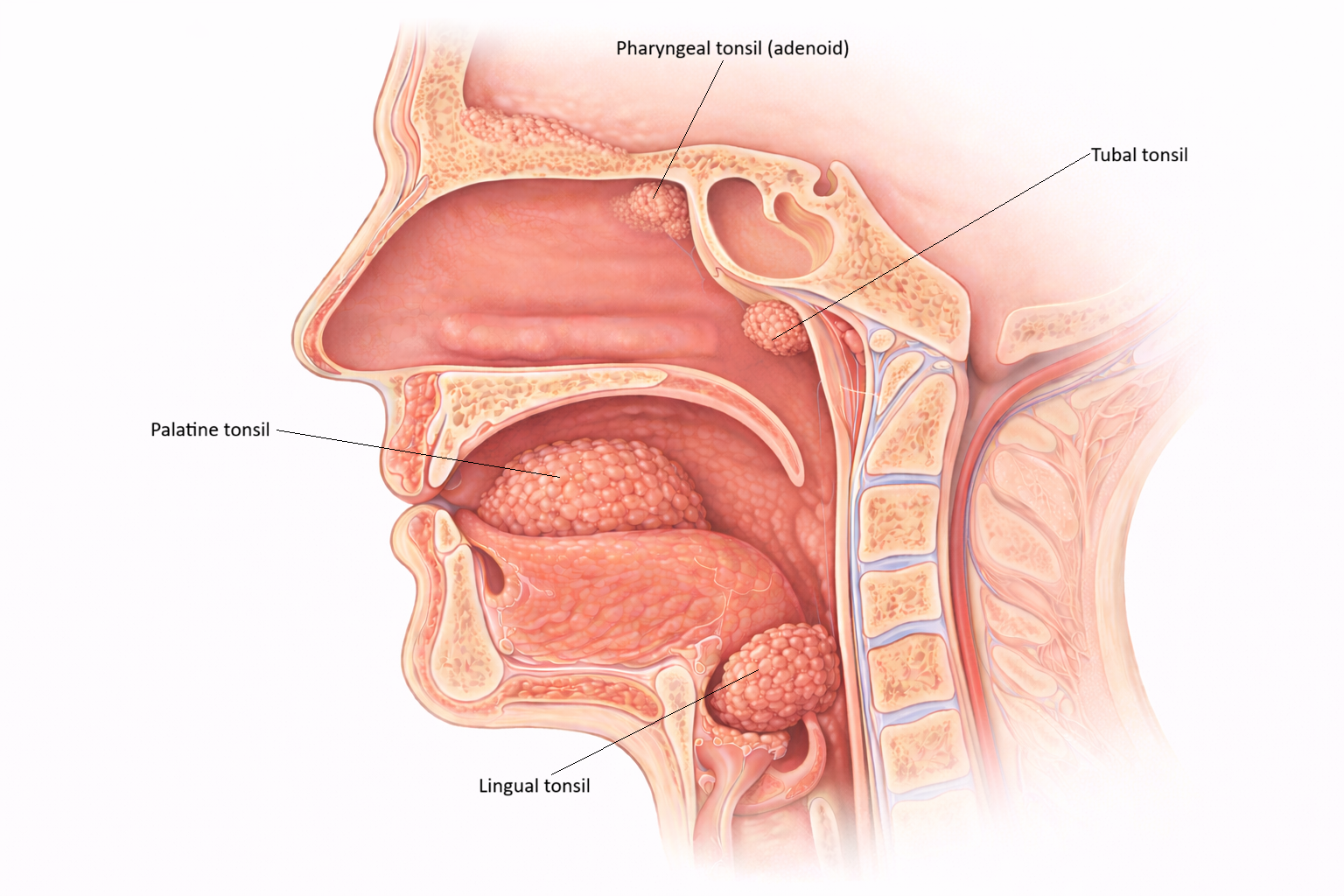
Image: The tonsils form a ring of lymphoid tissue around the nasopharynx and oropharynx, including the pharyngeal, tubal, palatine, and lingual tonsils. Positioned at the entrance to the respiratory and digestive tracts, they sample inhaled and ingested pathogens to initiate early immune responses. Tonsillar tissue simplified and slightly exaggerated for educational purposes.
Beyond the Basics
Types of Tonsils and Their Locations
Waldeyer’s ring is composed of several distinct tonsillar structures, each positioned to monitor antigens entering through the mouth or nose. Although they share a common immune function, their anatomy reflects the type of exposure they encounter most frequently.
Palatine tonsils are located on either side of the oropharynx between the palatoglossal and palatopharyngeal arches. These are the tonsils most commonly referred to in clinical practice and are frequently removed during tonsillectomy. Their deep crypts markedly increase surface area, improving antigen capture but also allowing bacteria and debris to accumulate, which contributes to recurrent infection.
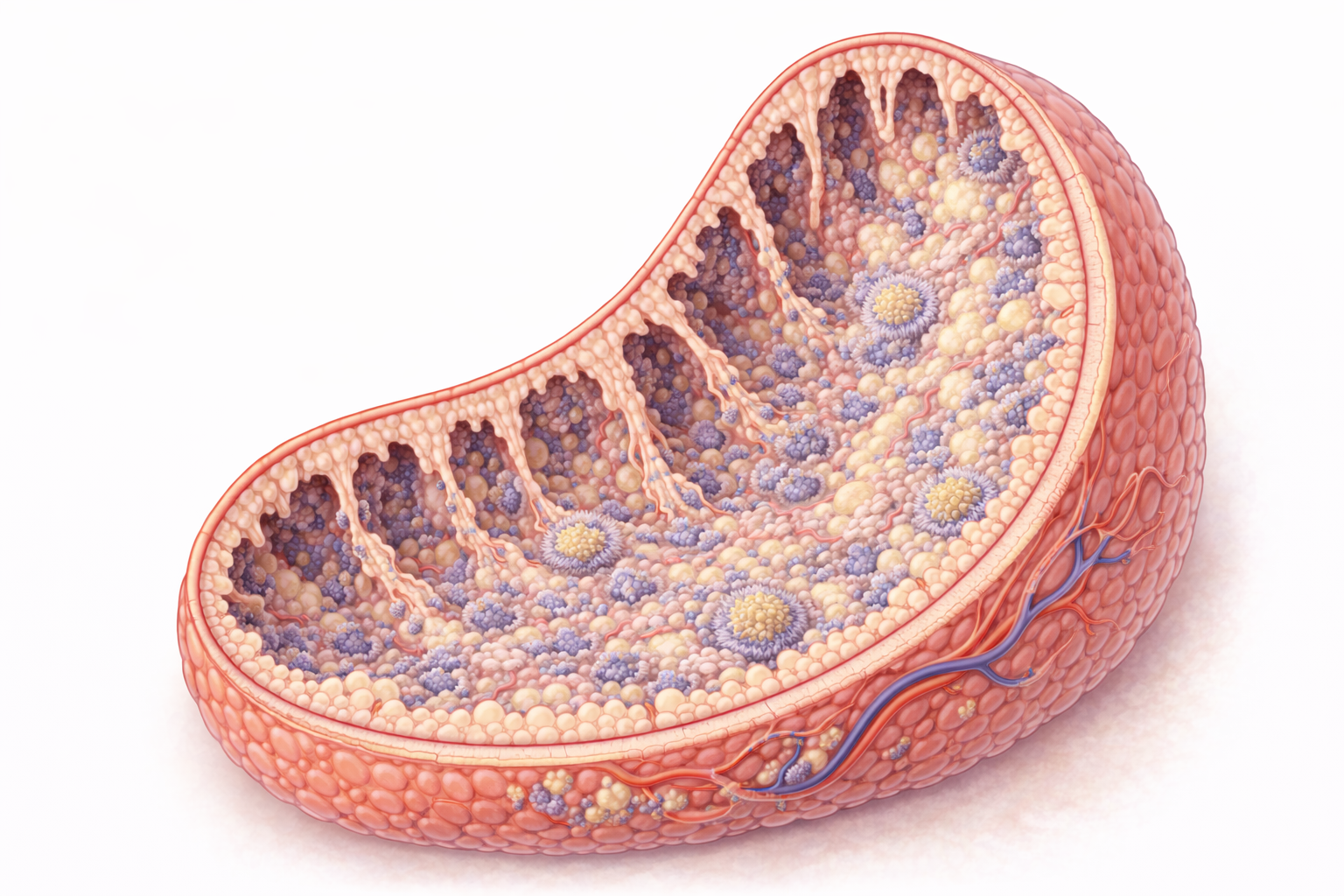
Image: Palatine tonsils contain deep, branching crypts lined by stratified squamous epithelium that is infiltrated by immune cells. These crypts increase surface area, allowing trapped pathogens to interact with underlying lymphoid tissue and initiate immune responses.
The pharyngeal tonsil, commonly called the adenoids, sits in the roof of the nasopharynx. It is covered by ciliated pseudostratified columnar epithelium, similar to the rest of the respiratory tract. This location allows continuous sampling of inhaled antigens and airborne pathogens before they reach the lower respiratory system.
Lingual tonsils are found at the base of the tongue. They consist of multiple small nodules of lymphoid tissue rather than a single mass. Their crypts are shallower than those of the palatine tonsils, which reduces debris retention while still supporting antigen exposure from ingested material.
Together, these tonsils form a continuous immunological ring that monitors the entry points of the respiratory and gastrointestinal systems.
Histological Structure
Tonsils share a common lymphoid architecture that supports rapid immune activation. Each tonsil contains organised lymphoid follicles with germinal centres, where B cells proliferate and differentiate following antigen exposure. These follicles are supported by a reticular connective tissue framework that allows immune cells to migrate and interact efficiently.
The epithelial covering varies according to tonsil type:
Palatine and lingual tonsils are lined by stratified squamous epithelium, suited to mechanical stress from food and speech
The pharyngeal tonsil is lined by ciliated respiratory epithelium, supporting mucociliary clearance
This variation ensures that each tonsil is structurally adapted to its local environment while maintaining immune function.
Mechanisms of Immune Activation
Antigens become trapped within tonsillar crypts or adhere to the epithelial surface. Dendritic cells sample these antigens and transport them into the underlying lymphoid tissue. There, antigens are presented to T lymphocytes, while B cells within follicles undergo clonal expansion and differentiation.
Activated B cells produce antibodies, particularly IgA, which plays a major role in mucosal defence by neutralising pathogens at epithelial surfaces. T cell activation supports antiviral and antibacterial responses and helps coordinate broader immune activity. Because this process occurs locally, immune responses can begin rapidly without requiring systemic activation.
Role in Childhood Immunity
Tonsillar tissue is most active during childhood, a period marked by frequent exposure to novel antigens. During this time, tonsils contribute to development of adaptive immune responses and establishment of immunological memory. Repeated antigen sampling helps train the immune system to respond effectively to common pathogens while maintaining tolerance to non-threatening exposures.
As immune memory becomes established, tonsillar tissue gradually decreases in size through a process known as involution. This reduction in adulthood reflects decreased reliance on tonsillar surveillance rather than loss of immune competence, as systemic and mucosal immune memory has already been established.
Clinical Connections
Tonsillar disease is common because tonsils sit directly at mucosal entry points where exposure to pathogens is frequent. Acute tonsillitis may be caused by viral or bacterial infection and often presents with sore throat, fever, dysphagia, and visibly enlarged or exudative tonsils. Chronic or recurrent tonsillitis occurs when repeated antigen exposure leads to ongoing inflammation and incomplete resolution between episodes.
Several clinical presentations are closely associated with tonsillar pathology:
Painful swallowing and fever during acute infection
Cervical lymphadenopathy accompanying active immune responses
Recurrent throat infections affecting nutrition, sleep, and school attendance
Airway compromise when tonsillar tissue becomes significantly enlarged
Adenoid hypertrophy is particularly relevant in paediatric populations. Enlargement of the pharyngeal tonsil can obstruct the nasopharynx, leading to mouth breathing, nasal speech, chronic nasal congestion, snoring, and obstructive sleep apnoea. Prolonged airway obstruction may affect sleep quality, behaviour, and growth, making early recognition important.
Tonsillectomy may be indicated when recurrent infection, chronic inflammation, or significant hypertrophy interferes with airway patency, swallowing, or quality of life. Enlargement of tonsillar tissue during infection is driven by lymphocyte proliferation within germinal centres as immune cells respond to antigen exposure. Although tonsils contribute to early immune defence, removal does not cause long-term immune deficiency, as immune memory and other lymphoid tissues continue to provide protection.
Concept Check
What is Waldeyer’s ring, and which tonsils does it include?
Why do tonsils contain crypts, and what functional advantage do they provide?
How do tonsils initiate immune responses to inhaled or ingested pathogens?
Why are tonsils particularly active during childhood?
What types of epithelium cover the different tonsils, and why do they differ?