THE PLACENTA: Structure & Function
The placenta is a temporary but highly specialised organ that supports fetal growth, development and survival throughout pregnancy. It forms the essential interface between maternal and fetal circulations, enabling nutrient transfer, gas exchange, waste removal and endocrine signalling. Beyond its transport functions, the placenta regulates immune tolerance, produces critical hormones and orchestrates key developmental processes that shape gestational health. Understanding placental structure and function is fundamental for interpreting pregnancy physiology, fetal development, maternal adaptations and pregnancy complications.
What You Need to Know
The placenta is a transient but highly specialised organ that forms the interface between maternal and fetal systems. It develops from two sources: the fetal chorionic villi and the maternal decidua of the uterus. Together, these components create a complex exchange surface that supports fetal growth while maintaining separation of maternal and fetal blood. This arrangement allows efficient transfer of gases, nutrients, and waste products without direct blood mixing.
Structurally, maternal blood is delivered into the intervillous space via spiral arteries, where it bathes the branching chorionic villi. Within these villi, fetal capillaries lie close to the maternal blood pool, separated only by the placental membrane. The thinness and large surface area of this membrane optimise diffusion and transport while still providing a controlled barrier. As pregnancy progresses, placental structure adapts to increasing fetal demands through villous branching and vascular remodelling.
Beyond exchange, the placenta functions as a powerful endocrine organ that regulates both pregnancy maintenance and maternal adaptation. It produces hormones that support the uterine environment, modulate maternal metabolism, and coordinate fetal development. Key placental roles include:
Gas and nutrient exchange, supplying oxygen and substrates while removing fetal waste
Endocrine regulation, through production of hormones that sustain pregnancy and alter maternal physiology
Immunological modulation, protecting the fetus while permitting selective immune transfer
Immunologically, the placenta balances protection with tolerance. It limits maternal immune activation against fetal tissue while allowing transfer of immunoglobulin G antibodies that provide passive immunity to the fetus. This selective permeability, combined with endocrine and transport functions, makes the placenta central to healthy pregnancy progression and fetal wellbeing.
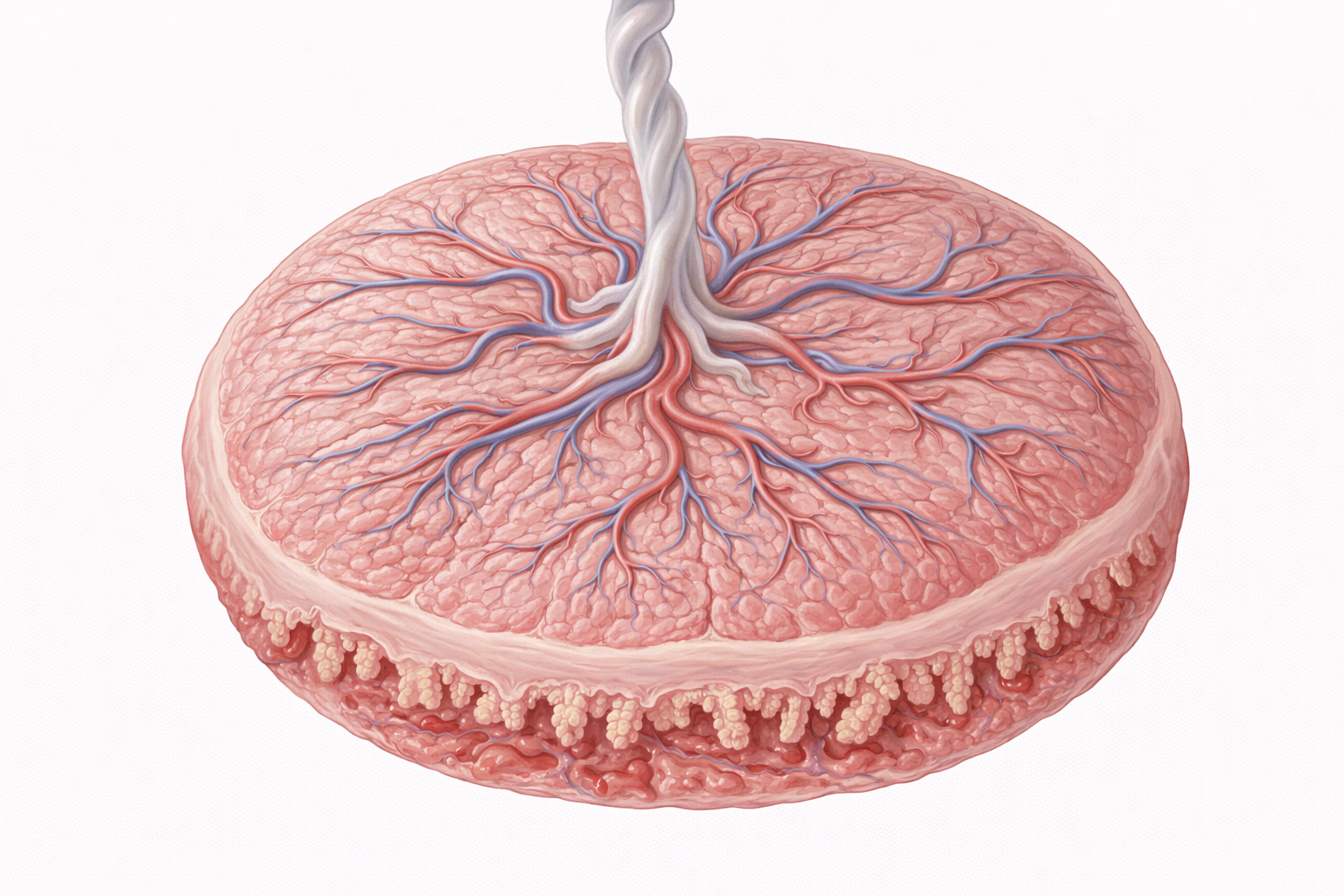
Image: The placenta is a temporary organ that forms during pregnancy, connecting the developing fetus to the uterine wall. It facilitates the exchange of oxygen, nutrients, and waste products between maternal and fetal blood, while also producing hormones that support pregnancy.
Beyond the Basics
Development and Structural Organisation
Placental development begins soon after implantation, when trophoblast cells differentiate into two specialised populations. Cytotrophoblasts form an inner cellular layer, while syncytiotrophoblasts fuse into a multinucleated outer layer that invades the maternal endometrium. This invasive syncytiotrophoblast establishes early maternal contact and initiates nutrient and gas exchange well before the fetal circulation is fully developed.
As pregnancy progresses, chorionic villi undergo extensive branching, dramatically increasing the surface area available for exchange. Each villus contains fetal capillaries embedded within a connective tissue core, bringing fetal blood into close proximity with maternal blood in the intervillous space. The maternal component of the placenta, the decidua basalis, develops from hormonally transformed endometrial stromal cells and anchors the placenta to the uterine wall. Mature placental tissue is organised into multiple lobules known as cotyledons, each supplied by a spiral artery and containing numerous villous trees that function as independent exchange units.
Maternal–Fetal Circulation and the Intervillous Space
Effective placental function depends on specialised maternal vascular remodelling early in pregnancy. Spiral arteries lose their muscular and elastic layers, transforming into low-resistance vessels capable of delivering large volumes of maternal blood into the intervillous space. This adaptation ensures steady perfusion of the chorionic villi and is essential for adequate fetal oxygen and nutrient supply.
Within the intervillous space, maternal blood bathes the chorionic villi without direct contact with fetal blood. Exchange occurs across the placental membrane, which consists of syncytiotrophoblast, a basement membrane, and fetal capillary endothelium. Deoxygenated blood leaves the fetus through two umbilical arteries, while oxygenated, nutrient-rich blood returns via a single umbilical vein. This parallel but separate circulation allows efficient exchange while preserving maternal and fetal blood integrity.
Placental Endocrine Function
By the end of the first trimester, the placenta assumes primary responsibility for hormonal support of pregnancy. Hormone production is largely driven by syncytiotrophoblasts and increases progressively as placental mass expands. Human chorionic gonadotropin supports the corpus luteum in early pregnancy, ensuring continued progesterone secretion until placental progesterone production is sufficient. This hormone is also the basis of pregnancy detection in clinical testing.
Progesterone produced by the placenta maintains the endometrial lining, suppresses uterine contractility, and contributes to immune tolerance of the fetus. Estrogens, particularly estriol, promote uterine growth, enhance placental blood flow, and prepare mammary tissue for lactation. Human placental lactogen modifies maternal metabolism by inducing insulin resistance and promoting lipolysis, ensuring a continuous glucose supply to the fetus while increasing maternal reliance on fat metabolism. In addition to these major hormones, the placenta produces corticotropin-releasing hormone, leptin, growth factors, and cytokines that influence fetal growth, maternal physiology, and the timing of labour.
Transport Mechanisms Across the Placenta
Transfer of substances across the placenta is highly selective and tightly regulated. Different transport mechanisms are employed depending on molecular size, charge, and physiological importance. Oxygen, carbon dioxide, and small waste products move by simple diffusion along concentration gradients. Glucose crosses the placenta by facilitated diffusion through specific transporters, ensuring fetal access to maternal energy supplies.
Essential nutrients such as amino acids, electrolytes, iron, and calcium are transported actively against concentration gradients, reflecting their importance for fetal growth and skeletal development. Maternal immunoglobulin G antibodies are transferred by receptor-mediated endocytosis, providing passive immunity that protects the newborn during early life. As pregnancy advances, the placental barrier becomes thinner, improving exchange efficiency to meet increasing fetal demands.
Immunological Protection and Maternal Tolerance
The placenta plays a central role in preventing immune rejection of the fetus, which is genetically distinct from the mother. Syncytiotrophoblasts do not express classical major histocompatibility complex class I molecules, reducing recognition by maternal immune cells. Local immune modulation within the decidua further supports tolerance through the activity of regulatory T cells and the release of anti-inflammatory cytokines.
This immune adaptation is selective rather than suppressive. Maternal defences against infection remain active, while fetal tissues are protected from immune attack. Transfer of maternal immunoglobulin G antibodies increases markedly in the third trimester, equipping the fetus with passive immunity that persists after birth. Together, these mechanisms highlight the placenta as both an immunological barrier and an active regulator of maternal–fetal immune balance.
Clinical Connections
Placental function is central to pregnancy outcomes, and disruption at any stage can have significant maternal and fetal consequences. When normal placental development or perfusion is impaired, the fetus may receive inadequate oxygen and nutrients despite otherwise normal maternal physiology. Many serious obstetric complications can be traced back to abnormal placental structure, vascular remodelling, or endocrine function rather than primary fetal disease.
One of the most critical processes is early spiral artery remodelling. Failure of this adaptation results in high-resistance uteroplacental blood flow, reducing placental perfusion. This underlies placental insufficiency and contributes to conditions such as intrauterine growth restriction and pre-eclampsia. Structural placental abnormalities also disrupt exchange and attachment, each with distinct clinical implications. Important placental pathologies include:
Placental insufficiency, leading to restricted fetal growth and reduced oxygen delivery
Placenta previa or accreta, where abnormal implantation increases haemorrhage risk
Placental abruption, involving premature separation that compromises fetal oxygenation and maternal stability
Placental hormones also influence maternal metabolic health. Gestational diabetes reflects an exaggerated response to placental hormone driven insulin resistance, particularly from human placental lactogen and related hormones. When maternal insulin secretion cannot compensate, hyperglycaemia develops, increasing risks for fetal overgrowth, birth complications, and long-term metabolic effects for both mother and child.
Examination of the placenta after birth can provide valuable insight into pregnancy outcomes. Findings such as infarction, inflammation, abnormal cord insertion, or vascular pathology often explain fetal growth patterns, preterm birth, or intrapartum compromise. Beyond diagnosis, understanding placental physiology informs key areas of care, including management of Rh incompatibility, assessment of medication transfer and fetal exposure, interpretation of fetal monitoring, and decisions around timing of delivery.
Concept Check
How do chorionic villi facilitate maternal–fetal exchange without mixing maternal and fetal blood?
What roles do hCG, progesterone and hPL play in pregnancy maintenance?
How does spiral artery remodelling support fetal oxygenation?
What mechanisms allow selective transfer of nutrients and antibodies across the placenta?
How can placental dysfunction contribute to pregnancy complications such as pre-eclampsia or fetal growth restriction?